Impact Factor
- Issue 14; 2026
- Issue 13; 2026
- Issue 12; 2026
- Issue 11; 2026
- Issue 10; 2026
- Volume 16; 2026
- Advance Articles
- Past Issues
- Cover Images
- Cover Suggestion
- Index & Coverage
- Special Issues
Introduction
Materials and Methods
Results and Discussion
Conclusions
Abbreviations
Supplementary Material
Acknowledgements
References
International Journal of Biological Sciences
International Journal of Medical Sciences
 Global reach, higher impact
Global reach, higher impact

Theranostics 2026; 16(12):6980-6987. doi:10.7150/thno.122256 This issue Cite
Research Paper
First-in-human ex-vivo validation of carbonic anhydrase IX-PET for high-risk renal cancer (CAT-VHL - PNRR-POC-2023-12377493)
Alessandro Larcher1,2 ![]() *, Fabrizia Gelardi3*, Lidija Antunovic3*, Annarita Savi3, Michela Olivieri3, Paolo Rainone3,4, Martina Sollini3,5, Rosa Maria Moresco3,4,6, Chiara Re1,2,5, Francesco Cei1,2,5, Federico Belladelli1,2,5, Giacomo Musso1,2,5, Lucia Salerno1,2,5, Francesco De Cobelli5,7, Nazario Tenace5,8, Maurilio Ponzoni5,8, Antonio Cigliola9, Paolo Verze10,11, Roberto Bertini1,2, Alberto Briganti1,2,5, Francesco Montorsi1,2,5, Umberto Capitanio1,2*, Andrea Salonia1,2,5*, Arturo Chiti3,5*
*, Fabrizia Gelardi3*, Lidija Antunovic3*, Annarita Savi3, Michela Olivieri3, Paolo Rainone3,4, Martina Sollini3,5, Rosa Maria Moresco3,4,6, Chiara Re1,2,5, Francesco Cei1,2,5, Federico Belladelli1,2,5, Giacomo Musso1,2,5, Lucia Salerno1,2,5, Francesco De Cobelli5,7, Nazario Tenace5,8, Maurilio Ponzoni5,8, Antonio Cigliola9, Paolo Verze10,11, Roberto Bertini1,2, Alberto Briganti1,2,5, Francesco Montorsi1,2,5, Umberto Capitanio1,2*, Andrea Salonia1,2,5*, Arturo Chiti3,5*
1. Department of Urology, Division of Oncology, Urological Research Institute, IRCCS Ospedale San Raffaele, Milan, Italy.
2. VHL Program, IRCCS Ospedale San Raffaele, Milan, Italy.
3. Department of Nuclear Medicine, IRCCS Ospedale San Raffaele, Milan, Italy.
4. Institute of Molecular Bioimaging and Physiology-IBFM, CNR, Segrate, Italy.
5. Vita-Salute San Raffaele University, Milan, Italy.
6. Department of Medicine and Surgery, University of Milano-Bicocca, Monza, Italy.
7. Department of Radiology, IRCCS Ospedale San Raffaele, Milan, Italy.
8. Department of Pathology, IRCCS Ospedale San Raffaele, Milan, Italy.
9. Department of Oncology, IRCCS Ospedale San Raffaele, Milan, Italy.
10. Department of Urology, AOU San Giovanni di Dio Ruggi d'Aragona, Salerno, Italy.
11. Università degli Studi di Salerno, Salerno, Italy.
*Equal contribution.
Received 2025-7-26; Accepted 2026-2-27; Published 2026-5-18
Abstract

Rationale: Carbonic Anhydrase IX (CAIX) positron emission tomography (PET) is an accurate and non-invasive imaging modality for the detection and characterisation of clear-cell renal cell carcinoma (ccRCC) but evidence in the setting of high-risk renal cancer is lacking. We conducted an exploratory investigation to integrate whole-body CAIX-PET imaging with tissue-level validation and to assess the potential impact of CAIX-PET on systemic staging in patients diagnosed with high-risk renal cancer.
Methods: Patients with cT3–cT4 or cN1 renal cancer scheduled for surgery underwent PET/CT imaging after intravenous administration of 37 MBq ±10% of [89Zr]Zr-girentuximab. Whole-body in-vivo was performed 5 ± 2 days following radiopharmaceutical injection, and surgical resection was planned 14 ± 2 days following radiopharmaceutical injection. Resected specimens were subsequently analyzed ex vivo using dedicated preclinical PET/CT imaging and correlated with histopathology and CAIX immunohistochemistry.
Results: No adverse events following [89Zr]Zr-girentuximab administration were recorded and the procedure was deemed non-relevant in terms of radiation exposure for the surgical team. At in-vivo imaging, CAIX-PET resulted positive in 2 patients with clear cell renal cell carcinoma and negative in 1 patient with chromophobe renal cell carcinoma. At ex-vivo imaging, images overlap allowed for the assessment of spatial co-localization of regions with increased radiopharmaceutical uptake and high expression of CAIX at immunohistochemistry. In 1 patient, focal uptake in the fourth rib at CAIX-PET was confirmed as metastatic ccRCC. In 1 patient, suspicious lymph nodes at standard imaging without PET uptake were negative at final pathology.
Conclusion: Our findings generate the hypothesis that CAIX-PET might yield crucial information on cancer aggressiveness and systemic staging with potential key diagnostic, therapeutic and prognostic implications for patients with high-risk renal cancer.
Keywords: renal cell carcinoma, carbonic anhydrase IX, positron-emission tomography, theranostics, tumor heterogeneity
Introduction
Clear cell renal cell carcinoma (ccRCC), the most common and most aggressive renal cancer subtype [1], is characterized by substantial biological heterogeneity and unpredictable metastatic behavior [2] . Conventional imaging does not capture spatial molecular variability in the primary and may fail to provide accurate systemic staging in case of metastatic disease.
Carbonic anhydrase IX (CAIX) represents a hallmark of ccRCC biology and a promising target for molecular imaging, currently under scrutiny for the diagnosis of clear cell renal cell carcinoma (ccRCC). The sensitivity and specificity of CAIX-PET were 86% and 87% in a phase 3 clinical trial assessing patients with an indeterminate cT1 renal mass elected for nephrectomy [4]. However, no evidence is available in the setting of high-risk renal cancer [5].
During cancer evolution and clonal de-differentiation, proximal-tubule cells might lose CAIX expression [6] either in the primary tumor or in distant metastases; hence preventing detection with CAIX-PET imaging. For this reason, with the intent to provide preliminary clinical data supporting the use of CAIX-PET in high-risk ccRCC, we conducted an exploratory investigation to integrate whole-body CAIX-PET imaging with tissue-level validation and to assess the potential impact of CAIX-PET on systemic staging in patients diagnosed with high-risk renal cancer.
Materials and Methods
First, we obtained approval by the Ethical Committee for early access program under compassionate use (Comitato Etico Territoriale Lombardia 1 - N°20-2024) and subsequently, we obtained approval by the Ethical Committee and AIFA - Agenzia Italiana del Farmaco for a phase 2 clinical trial (CAT-VHL - PNRR-POC-2023-12377493 trial; https://clinicaltrials.gov/study/NCT07171905).
We selected patients diagnosed with high-risk renal cancer, defined as stage cT3-cT4 or cN1 at conventional imaging and administered a single intravenous dose of the standard diagnostic activity (37 MBq ± 10%) of [89Zr]Zr-girentuximab, an anti-CAIX monoclonal antibody radiolabeled with Zirconium-89. Subsequently, all patients were subjected to whole-body imaging with a hybrid PET/CT scanner (GE Healthcare Omni Legend) on day 5 ± 2 after radiopharmaceutical administration. PET/CT scanner characteristics and acquisition parameters are described in Table S1.
Following the approval of a dedicated protocol for radioprotection by the institutional physics service, surgery was planned on day 14 ± 2 after radiopharmaceutical injection. This timing was chosen based on theoretical dosimetry estimates and the long half-life of Zirconium-89 (78.4 hours), with the intent to maximally reduce the exposure of the surgical team and at the same time to maximally increase the likelihood of detecting adequate activity in cancer tissue. Immediately after surgery, the renal specimens were initially fixed in formalin and subsequently sectioned along parafrontal planes to obtain slices suitable for the dimensions of the imaging equipment. The slices containing the lesion and adjacent renal parenchyma were then placed in sealed polyethylene specimen bags. Subsequently, we performed ex vivo studies using a preclinical CT and PET scanner (X-cube® and β-cube®, Molecubes, Gent, Belgium [7]). Each surgical specimen was placed on the scanner bed and first imaged with the preclinical CT scanner (X-cube®) in high-resolution mode for approximately three minutes. The bed was subsequently transferred to the preclinical PET scanner (β-Cube®) and scanned for a 180-minute acquisition. CT data were reconstructed with an isotropic pixel size of 200 µm using the ISRA algorithm, while PET data were reconstructed using the OSEM algorithm (10 iterations, isotropic voxel size 400 µm), including corrections for tracer decay and attenuation. Following imaging, specimens were processed for histopathological evaluation by an expert genitourinary pathologist.
Results and Discussion
Patients’ data are described in Table 1. No adverse events following [89Zr]Zr-girentuximab administration were recorded. Radiation exposure of the surgical team was negligible, with a maximal adsorbed dose of 0.018 mSv measured by cuff dosimeter; accordingly, the procedure was deemed non-relevant in terms of radiation exposure. Moreover, surgery was not technically influenced by exposure to the radiopharmaceutical in any way. In one case, a small accidental pleural opening occurred and required suturing. The event was largely anticipated owing to the location and dimension of the primary tumor. The patient had fever and transient acute respiratory failure treated with antibiotic and oxygen support (Clavien-Dindo 2). No major postoperative complications were recorded.
Patients’ characteristics.
| VARIABLE | CASE 1 | CASE 2 | CASE 3 | |
|---|---|---|---|---|
| General history | Age | 46 | 61 | 57 |
| Sex | M | M | M | |
| BMI | 24 | 27 | 26 | |
| Preoperative eGFR(ml/min/BSA) | 59 | 96 | 68 | |
| Conventional imaging | Side | R | L | L |
| Tumor size(cm) | 16 | 6 | 10 | |
| cT stage | cT3b | cT3a | cT2b | |
| cN stage | cN1 | cN0 | cN1 | |
| cM stage | cM0 | cM0 | cM0 | |
| CAIX-PET | Primary tumor | Positive | Positive | Negative |
| cN stage | cN0 | cN0 | cN0 | |
| cM stage | cM0 | cM1 | cM0 | |
| Surgery | Intervention | Radical Nephrectomy | Radical Nephrectomy | Radical Nephrectomy |
| Lymph-node dissection | Hilar and para-caval | No | Hilar and para-aortic | |
| Approach | Open surgery | Robotic surgery | Open surgery | |
| Intraoperative complications | Pleural lesion and pneumothorax | None | None | |
| Operative time(min) | 217 | 174 | 196 | |
| Hospital stay | Post-operative complications | Fever and acute respiratory distress syndrome | None | None |
| Clavien-Dindo classification | 2 | 0 | 0 | |
| Length of stay(days) | 10 | 3 | 7 | |
| Pathology | Histology | Clear cell | Clear cell | Chromophobe |
| Grade | 4 | 3 | 3 | |
| pT stage | pT3a | pT3a | pT3a | |
| pN stage | pN0 | pNx | pN0 | |
| pM stage | pMx | pM1 | pMx | |
| Necrosis | Yes | No | Yes | |
| LVI | Yes | No | Yes | |
| Sinus fat invasion | Yes | Yes | Yes | |
| Perirenal fat invasion | No | No | No | |
| Renal vein invasion | No | No | No | |
| Adrenal gland | Not infiltrated | Not infiltrated | Not infiltrated | |
| Margins | R0 | R0 | R0 | |
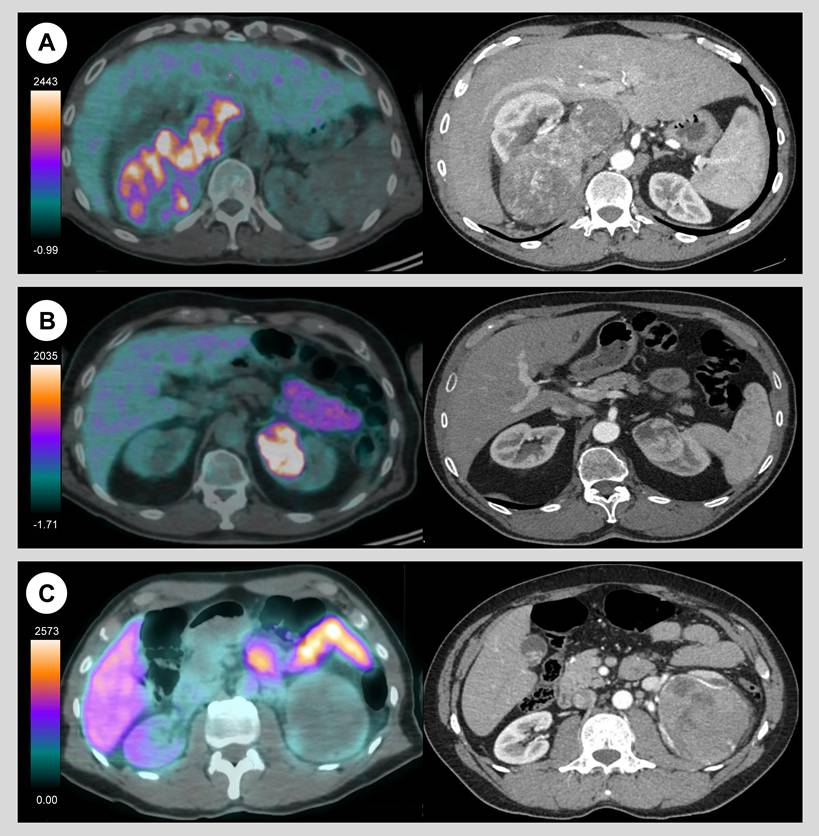
CAIX-PET resulted positive in two cases where in-vivo studies exhibited intense albeit spatially heterogeneous radiopharmaceutical uptake in primary tumour. Pathology confirmed ccRCC subtype (Figure 1A and 1B). Conversely, CAIX-PET resulted negative in a third case, and in-vivo study exhibited no uptake in the primary. Pathology revealed chromophobe subtype (Figure 1C). All cases were high-risk renal cancer with either high stage and high grade features.
Axial in-vivo CAIX-PET/CT (left) and standard contrast-enhanced CT (right) images in three patients with high-risk renal cancer. CAIX-PET demonstrated significant albeit spatially heterogeneous uptake in the primary renal tumor in two cases -right kidney (A) and left kidney (B)- later confirmed as pT3a renal cell carcinoma at final pathology. In one case (C), CAIX-PET was negative, with no significantly detectable tumor uptake. This finding was confirmed at final pathology as a pT3a chromophobe tumor.
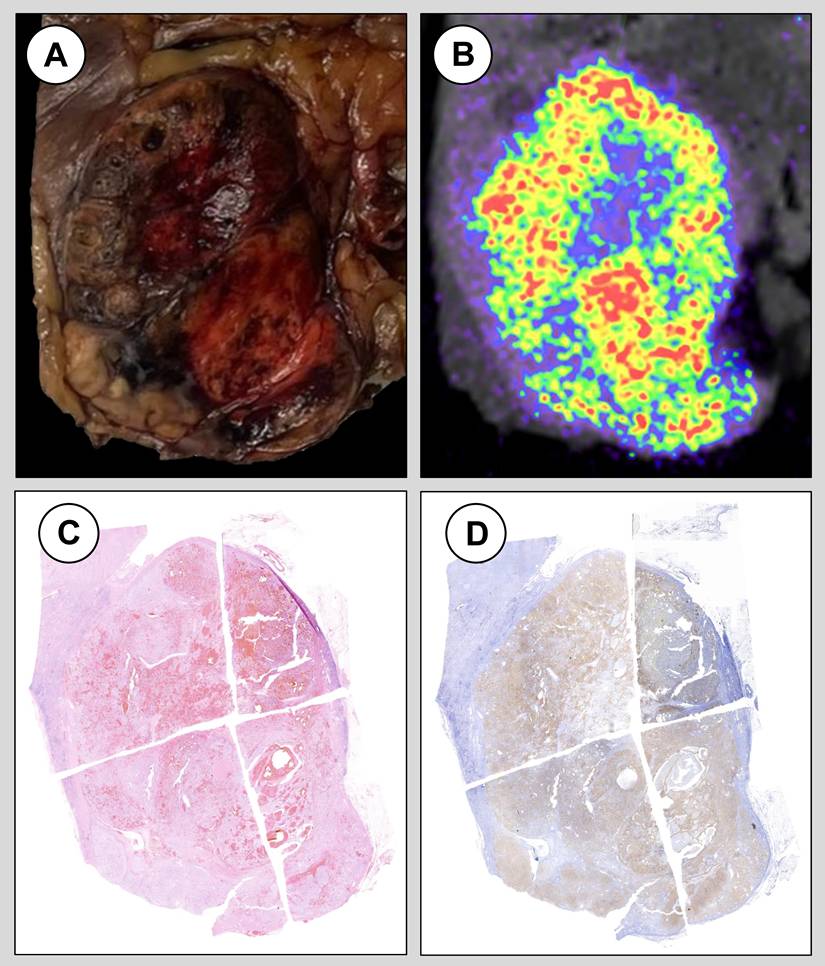
Images overlap allowed for the assessment of spatial co-localization of regions with increased radiopharmaceutical uptake and high expression of CAIX at immunohistochemistry (Video 1 and Figure S2). These regions were populated by viable cancer cells with abundant clear cell cytoplasm showing relatively aggressive features such as nucleolar grade 2 and 3 [8]. Consistently, regions with no radiopharmaceutical uptake were also CAIX negative at immunohistochemistry staining and were consistent with areas of fibrous and acellular myxoid degeneration that are often present in ccRCC. Of note, CAIX staining intensity and distribution was homogeneous in neoplastic areas with different architectural growth pattern but similar morphological features.
Macroscopic examination of the surgical specimen (A), ex-vivo imaging at preclinical PET/CT (B), hematoxylin and eosin staining (C) and immunohistochemistry staining for CAIX (D) in a patient diagnosed with a pT3a G3 clear cell renal cell carcinoma following robot-assisted radical nephrectomy.
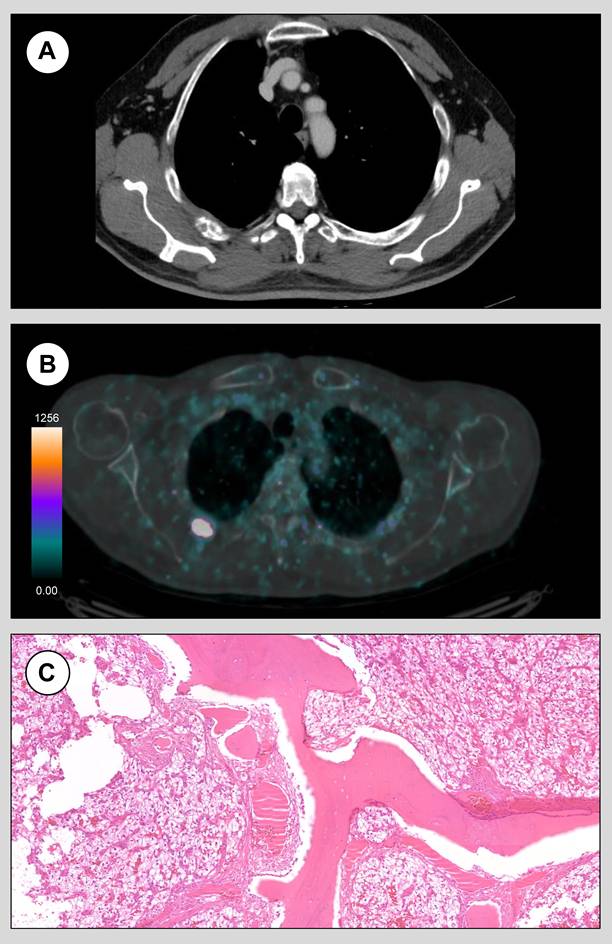
Whole body in-vivo CAIX-PET findings led to a significant revision of the initial staging. A case of cT3a cN0 cM0 renal cancer at standard imaging (Figure 3A) has been upstaged from cM0 to cM1 because of a pathological uptake at the fourth rib detected at CAIX-PET (Figure 3B) consistent with positive finding in the primary. Following multidisciplinary team discussion, the patient was elected for surgical resection of the rib lesion, and pathology confirmed a ccRCC metastasis (Figure 3C). Conversely, a case of cT2b cN1 cM0 renal cancer at standard imaging has been downstaged from cN1 to cN0 because of the absence of any uptake in the retroperitoneal lymph nodes at CAIX-PET despite positive finding in the primary. Final pathology confirmed pN0 disease and no nodal recurrence was detected at 12-months follow-up.
Axial standard chest CT images (A) and CAIX-PET images (B) of case 2. CAIX-PET prompted the reclassification from cM0 to cM1 by detecting pathological radiopharmaceutical uptake in the fourth rib. Following surgical metastasectomy, final pathology confirmed the presence of osseous trabeculae interspersed with richly vascularized neoplastic tissue composed of cells with abundant clear cytoplasm, consistent with metastatic ccRCC.
The novelty and uniqueness of these findings deserve special consideration. With respect to intra-tumoral heterogeneity, CAIX-PET can discriminate different regions within the same tumor with distinct and peculiar pathologic features. Our results highlight that the negligible uptake at CAIX-PET in certain portions of the tumor should not be regarded as false-negative outcome owing to sub-optimal radiopharmaceutical pharmacokinetics, but rather as true negative outcome owing to the lack of target expression at cellular level. Of note, false negative results of CAIX-PET are biologically plausible in case of high-risk localized or metastatic ccRCC without CAIX expression, and the frequency of this event cannot be determined based on our limited sample.
These observations might propel novel research lines with respect to relevant unmet clinical needs in the care of ccRCC patients. For instance, renal biopsy fails to provide a diagnosis in 10% of the cases [9], due to sampling of uninformative tissue. In this setting, CAIX-PET image-guided biopsy could reduce the rate of non-diagnostic biopsies by targeting the most informative areas of the tumor. Moreover, pre-treatment CAIX-PET-based estimation of cancer aggressiveness might justify a more demolitive surgical strategy such as radical instead of partial nephrectomy [9], ultimately reducing the risk of recurrence [10] in surgical candidates or might identify areas requiring radiation boost with supplemental dose in comorbid patients elected for external beam radiation therapy [11,12]. Finally, in the context of the ongoing development of novel theranostic agents for ccRCC [13,14], the pre-therapeutical identification of portions with limited radiopharmaceutical uptake could have critical implications with respect to dosimetry planning, as these instances have intrinsic risk of undertreatment.
With respect to detection of ccRCC metastases, better strategies to capture oligometastatic disease are critically needed, since most renal cancer metastases are asymptomatic, and fewer than 20% of cM+ renal cancer patients develop signs or symptoms [3]. Current international guidelines do not support the use of any nuclear imaging modality for renal staging [9] given the limitations of available radiopharmaceuticals. Specifically, the accuracy of [18F]F-deoxyglucose (FDG) is low, and the evidence supporting the use of prostate-specific membrane antigen (PSMA) [15], [99TC]TC-sestamibi [16] or [18F]F-azomycin arabinoside [17] is controversial. Remarkably, while treatment with systemic agents is mandatory in case of high metastatic burden, patients with oligometastatic disease are the ideal candidates for alternative strategies, including initial surveillance [18] or surgery of the primary together with metastasectomy [19]. Precise staging of the lymph nodes is even more problematic, since most clinically suspicious and enlarged nodes at standard imaging (cN1) are falsely positive (pT0) owing to the interaction between cancer and immune system [20] and trial specifically designed to test other radiopharmaceutical for the detection of lymph node involvement in renal cancer yielded negative results [17]. Consequently, CAIX-PET might support surgeons at planning the most appropriate lymph node dissection template [21].
This report stands out for its novelty and uniqueness, nonetheless it is inherently limited by its pilot and explorative nature. Therefore, the current sample size prevents any aggregate quantitative or comparative analysis.
Conclusions
Our findings generate the hypothesis that CAIX-PET might yield crucial information on cancer aggressiveness and systemic staging. Formal testing in clinical trials with adequate sample size and longitudinal evaluation of oncologic outcomes is needed to provide recommendations on the clinical benefit of CAIX-PET in high-risk renal cancer.
Abbreviations
CAIX: Carbonic Anhydrase IX
PET: Positron Emission Tomography
ccRCC: Clear Cell Renal Cell Carcinoma
Zr: Zirconium
MBq: Megabecquerel
mSv: Millisieverts
F: Fluorine
TC: Technetium
Supplementary Material
Supplementary material, (Supplementary Table 1 and Supplementary Figures 1 and 2), accompanies this manuscript and forms an integral part of the submission.
Video 1.
Acknowledgements
The authors Acknowledge Telix Pharmaceuticals for providing [89Zr]Zr-girentuximab as part of early access program. Moreover, the Authors acknowledge Daniela Canibus, Sabrina Bettini and Floriana Iannace for logistic support.
Funding
This study is funded by the European Union - Next Generation EU - NRRP M6C2 - Investment 2.1 Enhancement and strengthening of biomedical research in the NHS - PNRR-POC-2023-12377493; cup master C43C24000360007.
Authors' contributions
Study conception and design: Alessandro Larcher, Fabrizia Gelardi, Lidija Antunovic, Umberto Capitanio, Andrea Salonia, Arturo Chiti.
Acquisition of data: Alessandro Larcher, Fabrizia Gelardi, Lidija Antunovic, Annarita Savi, Michela Olivieri, Paolo Rainone, Martina Sollini, Chiara Re, Francesco Cei, Federico Belladelli, Giacomo Musso, Lucia Salerno, Francesco De Cobelli, Nazario Tenace, Antonio Cigliola, Paolo Verze, Roberto Bertini, Umberto Capitanio, Arturo Chiti.
Analysis and interpretation of data: Alessandro Larcher, Fabrizia Gelardi, Lidija Antunovic, Annarita Savi, Michela Olivieri, Paolo Rainone, Nazario Tenace, Arturo Chiti.
Drafting of the manuscript: Alessandro Larcher.
Critical revision of the manuscript for important intellectual content: Fabrizia Gelardi, Lidija Antunovic, Annarita Savi, Michela Olivieri, Paolo Rainone, Martina Sollini, Chiara Re, Francesco Cei, Federico Belladelli, Giacomo Musso, Lucia Salerno, Rosa Maria Moresco, Francesco De Cobelli, Nazario Tenace, Maurilio Ponzoni, Antonio Cigliola, Paolo Verze, Roberto Bertini, Alberto Briganti, Francesco Montorsi, Umberto Capitanio, Andrea Salonia, Arturo Chiti.
Obtaining funding: Alessandro Larcher, Fabrizia Gelardi, Lidija Antunovic, Chiara Re, Francesco Cei, Federico Belladelli.
Supervision: Francesco Montorsi, Andrea Salonia, Rosa Maria Moresco, Arturo Chiti.
Data availability
The data generated in the current study are publicly available (DOI: 10.5281/zenodo.19050017).
Simultaneous presentation and publications
Part of the findings presented within this study has been accepted for presentation at the 2026 European Association of Urology Annual Meeting as congress abstract (https://www.sciencedirect.com/science/article/pii/S0302283826005233?via%3Dihub).
Artificial intelligence
The authors declare that no artificial intelligence tools were used in the generation of data, data analysis, or image production. Artificial intelligence-assisted language tools were used solely to improve the clarity and linguistic quality of the manuscript and to provide the similarity and images integrity screening report. All scientific content, interpretation, and conclusions remain the sole responsibility of the authors.
Competing Interests
Alessandro Larcher discloses a restricted research grant from VHL Alliance to support the project “Investigation of treatment targets and tumour heterogeneity in Von Hippel–Lindau (VHL)-related renal cancer” and consulting activity including advisory board participation for Telix Pharmaceuticals and Merck Sharp & Dohme.
Fabrizia Gelardi discloses support by a restricted research grant from AIRC (Italian Association for Cancer Research) for the project “Investigator Grant 2019-23596” awarded to Arturo Chiti.
Umberto Capitanio discloses a restricted research grant from the Italian Ministry of Health and the European Union for the project “PNRR-MR1-2022-12375818”, consulting activity including honoraria for lectures, travel support and advisory board participation for Merck Sharp & Dohme and role as member of European Association of Urology Guidelines Panel on Renal Cancer.
Arturo Chiti discloses consulting activity including honoraria for lectures and advisory board participation for Telix Pharmaceuticals, Novartis, Sirtex, General Electric Healthcare, Bracco, Blue Earth Diagnostics and InnovaRadi Therapeutic.
References
1. Larcher A, Campi R, Bex A. et al. Epidemiology of Renal Cancer: Incidence, Mortality, Survival, Genetic Predisposition, and Risk Factors. Eur Urol. 2025.
2. Mitchell TJ, Turajlic S, Rowan A. et al. Timing the Landmark Events in the Evolution of Clear Cell Renal Cell Cancer: TRACERx Renal. Cell [Internet]. 2018;173:611-623.e17 Available at: http://eutils.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&id=29656891&retmode=ref&cmd=prlinks
3. Larcher A, Fallara G, Rosiello G. et al. Cytoreductive Nephrectomy in Metastatic Patients with Signs or Symptoms: Implications for Renal Cell Carcinoma Guidelines. European Urology [Internet]. 2020; 1-6. Available at: https://doi.org/10.1016/j. eururo. 2020 05.014
4. Shuch B, Pantuck AJ, Bernhard J-C. et al. [89Zr]Zr-girentuximab for PET-CT imaging of clear-cell renal cell carcinoma: a prospective, open-label, multicentre, phase 3 trial. Lancet Oncol. 2024;25:1277-87
5. Larcher A, Gelardi F, Montorsi F, Capitanio U, Chiti A. Molecular imaging targeting carbonic anhydrase IX for CCRCC: more than meets the eye. Lancet Oncol. 2024.
6. Büscheck F, Fraune C, Simon R. et al. Aberrant expression of membranous carbonic anhydrase IX (CAIX) is associated with unfavorable disease course in papillary and clear cell renal cell carcinoma. Urol Oncol: Semin Orig Investig. 2018;36:531.e19-531.e25
7. Presotto L, Spangler-Bickell M, Belloli S. et al. 3D Spatial resolution proprieties of Molecubes β-Cube: characterization with different isotopes. 2019 IEEE Nucl Sci Symp Méd Imaging Conf (NSSMIC). 2019 00: 1-2
8. Moch H, Cubilla AL, Humphrey PA, Reuter VE, Ulbright TM. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur Urol. 2016;70:93-105
9. Ljungberg B, Albiges L, Abu-Ghanem Y. et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur Urol. 2022;82:399-410
10. Martini A, Turri F, Barod R. et al. Salvage Robot-assisted Renal Surgery for Local Recurrence After Surgical Resection or Renal Mass Ablation: Classification, Techniques, and Clinical Outcomes. European Urology [Internet]. 2021 Available at: http://eutils.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&id=34088520&retmode=ref&cmd=prlinks
11. Siva S, Bressel M, Sidhom M. et al. Stereotactic ablative body radiotherapy for primary kidney cancer (TROG 15.03 FASTRACK II): a non-randomised phase 2 trial. Lancet Oncol. 2024;25:308-16
12. Ali M, Mooi J, Lawrentschuk N. et al. The Role of Stereotactic Ablative Body Radiotherapy in Renal Cell Carcinoma. Eur Urol. 2022;82:613-22
13. Muselaers CHJ, Boers-Sonderen MJ, Oostenbrugge TJ van. et al. Phase 2 Study of Lutetium 177-Labeled Anti-Carbonic Anhydrase IX Monoclonal Antibody Girentuximab in Patients with Advanced Renal Cell Carcinoma. Eur Urol. 2016;69:767-70
14. Hasanov E, Flynt L, Tidwell RS. et al. Phase 1b/2 study of combination 177 Lu girentuximab plus cabozantinib and nivolumab in treatment naïve patients with advanced clear cell RCC. J Clin Oncol. 2023;41:TPS4605-TPS4605
15. Rizzo A, Racca M, Dall’Armellina S. et al. The Emerging Role of PET/CT with PSMA-Targeting Radiopharmaceuticals in Clear Cell Renal Cancer: An Updated Systematic Review. Cancers. 2023;15:355
16. Basile G, Fallara G, Verri P. et al. The Role of 99mTc-Sestamibi Single-photon Emission Computed Tomography/Computed Tomography in the Diagnostic Pathway for Renal Masses: A Systematic Review and Meta-analysis. Eur Urol. 2024;85:63-71
17. Capitanio U, Pepe G, Incerti E. et al. The role of 18F-FAZA PET/CT in detecting lymph node metastases in renal cell carcinoma patients: a prospective pilot trial. European Journal of Nuclear Medicine and Molecular Imaging [Internet]. 2021 Available at: https://www.scopus.com/inward/record.uri?eid=2-s2.0-85087571694&doi=10.1007%2fs00259-020-04936-2&partnerID=40&md5=e207fb08eb008e6fba1b7cd22b6d2268
18. Rini BI, Dorff TB, Elson P. et al. Active surveillance in metastatic renal-cell carcinoma: a prospective, phase 2 trial. Lancet Oncol. 2016;17:1317-24
19. Dabestani S, Marconi L, Hofmann F. et al. Local treatments for metastases of renal cell carcinoma: a systematic review. Lancet Oncol [Internet]. 2014;15:e549-61 Available at: http://dx.doi.org/10.1016/S1470-2045(14)70235-9
20. Muttin F, Pecoraro A, Larcher A. et al. Predictive and prognostic effect of inflammatory lymphadenopathies in renal cell carcinoma. World J Urol. 2019;37:701-8
21. Rosiello G, Scilipoti P, Larcher A. et al. Neglected lymph nodal metastases in patients with renal cancer: when to extend the anatomical template of lymph node dissection during nephrectomy. World J Urol. 2023;41:1573-9
Author contact
![]() Corresponding author: Alessandro Larcher, MD, VHL Program, Department of Urology, Division of Oncology, Urological Research Institute, IRCCS Ospedale San Raffaele, Via Olgettina 60, 20132 Milan, Italy, Tel. +39 02 2643 4121, E-mail: larcher.alessandroit.
Corresponding author: Alessandro Larcher, MD, VHL Program, Department of Urology, Division of Oncology, Urological Research Institute, IRCCS Ospedale San Raffaele, Via Olgettina 60, 20132 Milan, Italy, Tel. +39 02 2643 4121, E-mail: larcher.alessandroit.