Impact Factor
- Issue 14; 2026
- Issue 13; 2026
- Issue 12; 2026
- Issue 11; 2026
- Issue 10; 2026
- Volume 16; 2026
- Advance Articles
- Past Issues
- Cover Images
- Cover Suggestion
- Index & Coverage
- Special Issues
Introduction
Typical MNAs for living organism...
MNAs integrated with living...
Challenges and perspectives
Acknowledgements
References
International Journal of Biological Sciences
International Journal of Medical Sciences
 Global reach, higher impact
Global reach, higher impact

Theranostics 2021; 11(20):10012-10029. doi:10.7150/thno.66478 This issue Cite
Review
Microneedle arrays integrated with living organisms for smart biomedical applications
Bo Cai1,5#, Yusheng Gong2,3#, Zheng Wang4,5 ![]() , Lin Wang1,5
, Lin Wang1,5 ![]() , Wei Chen2,3
, Wei Chen2,3 ![]()
1. Department of Clinical Laboratory, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430022, China.
2. Department of Pharmacology, School of Basic Medicine, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430030, China.
3. Hubei Key Laboratory for Drug Target Research and Pharmacodynamic Evaluation, Huazhong University of Science and Technology, Wuhan 430030, China.
4. Department of Gastrointestinal Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430022, China.
5. Research Center for Tissue Engineering and Regenerative Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430022, China.
#These authors contributed equally to this work.
Received 2021-8-25; Accepted 2021-10-2; Published 2021-10-25
Abstract

Various living organisms have proven to influence human health significantly, either in a commensal or pathogenic manner. Harnessing the creatures may remarkably improve human healthcare and cure the intractable illness that is challenged using traditional drugs or surgical approaches. However, issues including limited biocompatibility, poor biosafety, inconvenience for personal handling, and low patient compliance greatly hinder the biomedical and clinical applications of living organisms when adopting them for disease treatment. Microneedle arrays (MNAs), emerging as a promising candidate of biomedical devices with the functional diversity and minimal invasion, have exhibited great potential in the treatment of a broad spectrum of diseases, which is expected to improve organism-based therapies. In this review, we systemically summarize the technologies employed for the integration of MNAs with specific living organisms including diverse viruses, bacteria, mammal cells and so on. Moreover, their applications such as vaccination, anti-infection, tumor therapy and tissue repairing are well illustrated. Challenges faced by current strategies, and the perspectives of integrating more living organisms, adopting smarter materials, and developing more advanced technologies in MNAs for future personalized and point-of-care medicine, are also discussed. It is believed that the combination of living organisms with functional MNAs would hold great promise in the near future due to the advantages of both biological and artificial species.
Keywords: microneedle, living organism, smart integration, vaccination, anti-infection, cell-based therapy, cell and secretion delivery
Introduction
Numerous living organisms play significant roles in human health, some of which develop commensalism with human beings (e.g., gut microbes that extensively interact with the health of the host [1, 2]), while others would cause diseases (e.g., pathogenic parasitosis [3]). Due to the development of biological and material science, various organisms have been harnessed and utilized directly or in a modified manner to improve human healthcare. One famous successful case is the invention of live-attenuated vaccines [4]. Since the inoculation of cowpox that was popularized by Edward Jenner in the 18th century and the observation of attenuated principles for bacteria by Louis Pasteur, attenuated viruses or bacteria vaccinated to induce acquired immunity and establish immune prevention have saved countless lives [5, 6]. Some other living organisms have also been employed to develop novel therapeutic strategies for the diseases that are difficult to cure by traditional treatments. For instance, reconstitution or transplantation of microbes in the gut was able to relieve symptoms of recurrent clostridium difficile infection, Crohn's disease, ulcerative colitis, and so on [7-9]. Other successes include cell-based therapies that use autologous/allogeneic adult cells or stem cells (such as mesenchymal stem cells (MSCs) or induced pluripotent stem cells (iPSCs)) or function-engineered cells to repair injured or pathological tissues or organs, some of which have been applied in diseases relating to heart, liver, kidney, skeleton, nerve, eye, and so on [10-12]. Therapies using engineered immune cells have achieved remarkable success in treating cancers like leukemia and melanoma [13, 14]. Based on the discussion above, living organism-based therapy has become one of the most important subcategories in the field of biological medicine, undoubtedly attracting increasing attention from the entire world.
Compared to traditional therapies based on drugs or surgery, employing living organisms enables long-term disease treatment as a result of continuous interaction between the creatures and human bodies. Some of them persistently produce secretions such as cytokines, triggering protection or repairing, while others target specific cells or lesions for antigen or drug delivery. Furthermore, the abilities of proliferation and differentiation of some organisms (mainly stem cells) exhibited the promising potential to repair or replace cells or tissues that have lost functions when injured or in pathological states [15-17]. However, therapies using living organisms encounter several challenges: (1) Viability and safety. On one hand, the colonization of exogenous creatures into the human body confronts the immunological rejection from the host which hinders their survival. On the other hand, the organisms may proliferate out of control, and thus leading to tumorigenesis/parasitosis, or severe immune reaction to threaten lives [18, 19]. (2) Inconvenience and low compliance. Currently, therapeutic organisms are mainly delivered via bolus injection (e.g., vaccination [20] or cancer therapy [21]), scaffold transplantation (e.g., the use of cardiac patches [22]), or even surgical methods [23], which presents challenges toward personalized medicine at home or anywhere besides hospitals, and thus compromising patient compliance, greatly impeding their translation to clinical applications. Therefore, a safe and easy-to-use treatment regime that does not require professionals or specialized facilities is highly demanded.
With the development of novel materials and micromachining techniques, the emerging microneedle technology has become a promising candidate to treat various diseases in a minimally invasive manner without sophisticated equipment or specific professionals [24-27]. Microneedle array (MNA) is a piece of a substrate (mm2 to cm2 scale) containing an array of needles (a few to several hundred tips in total) with diverse mechanical and physicochemical properties. The individual needle on MNAs is well-shaped (e.g., cone or pyramid) with the length ranging from 200 to 1500 μm, and the diameter is around 250 to 600 μm [28, 29]. By integrating with biosensing systems or drug formulations, MNAs have been widely applied in biomarker detection (e.g., interstitial fluid or blood detection based on chemical, electrochemical or immune strategies) and specific drug delivery (such as delivering small molecules, peptides, proteins, oligonucleotides, nanoparticles, and so on) [30-32]. With advantages of minimal invasion, easy operation and bioresponsive delivery strategies, MNAs significantly benefit personal drug administration and improves patient compliance, and therefore demonstrating excellent strategies to meet challenges raised in current therapies using living organisms.
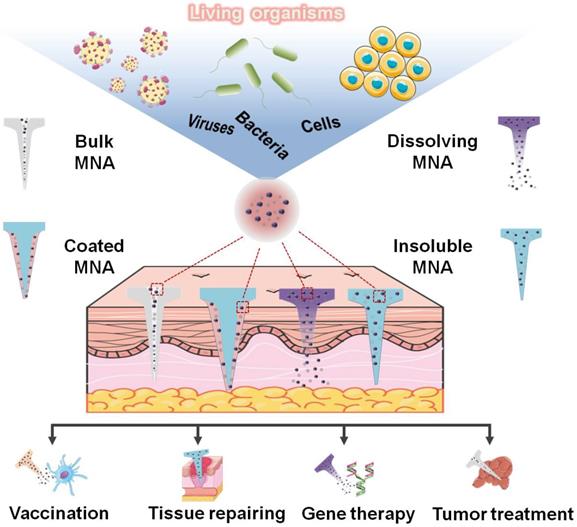
In this review, we systemically summarize the combinative systems of MNAs and living organisms, with specific biological species including diverse viruses, bacteria, mammal cells, and so on. Moreover, their applications such as vaccination, anti-infection, tumor therapy, and tissue repairing are well illustrated (Figure 1). Initially, we briefly introduce the specific classification and materials of MNAs used to integrate organisms. Subsequently, detailed integration strategies using the living organism and MNAs, and their corresponding applications for drug delivery and disease treatment are categorized according to the species of the organisms (i.e., virus, bacteria and mammal cells). Finally, we highlight the challenges faced by current strategies, and the perspectives including more living organisms, smarter materials and advanced novel technologies are discussed in-depth.
Specific living organisms including diverse viruses, bacteria, and mammal cells are integrated into MNAs and are widely applied in the fields of vaccination, tissue repairing, gene therapy, tumor treatment, and so on.
Typical MNAs for living organism integration
Strategies based on organism-MNA combination are mainly divided into two categories: (1) Directly applying living organisms into tissues/organs to induce repairing effects or the immune response. (2) Utilizing the secretion of living organisms to mediate metabolism or eradicate pathological cells/bacteria. Given the different cargoes (living species or their secretion) that needed to be delivered, MNA forms with distinct constitutions and working mechanisms are optimized. Moreover, the material selection for organism-integrated MNA fabrication should include the following features: (1) Suitable stiffness to ensure tissue penetration. (2) Excellent biocompatibility with minimal damage to the hosts and the integrated organisms. (3) Sufficient loading capacity of therapeutic agents for disease treatment.
Currently, there are mainly four types of MNAs, including bulk, coated, dissolving and insoluble MNAs. Each type of these MNAs adopts specific materials for fabrication and has its own unique delivery profile [32, 33], and they can be employed flexibly according to the requirement of integrating different organisms for special applications.
Bulk MNAs are mainly made of stiff materials such as metal (e.g., stainless steel), silicon and stiff polymers (e.g., poly(L-lactic acid)) with or without channels inside the MNAs. They are able to form micro-holes on the surface of target tissues to facilitate the therapeutic agents' transport. Among all types of MNAs, bulk MNAs display the highest mechanical strength, ensuring successful insertion and thus guaranteeing the delivery efficiency. Therefore they are widely employed for virus/bacteria-based vaccination.
Differently, coated and dissolving MNAs would dissolve into target tissues to release the encapsulated organisms after penetration. For coated MNAs, agents such as drugs or regulatory factors are directly deposited on the surface of MNA tips, which enables well mixture of the payload with interstitial fluid (ISF) to improve their diffusion into target locations. Meanwhile, dissolving MNAs are made of dissolvable materials (e.g., saccharides) that encapsulate therapeutic agents inside. After inserting into tissues, the whole microneedles are dissolved in ISF and release the payloads. In order to trigger ignorable immunogenicity or toxicity when degraded, and to effectively maintain the viability of organisms in MNAs, natural extracts like carboxymethyl cellulose (CMC), hyaluronic acid (HA) and saccharides (e.g., dextran, sucrose, maltose), or synthesized polymers such as polyvinyl alcohol (PVA), polyvinyl pyrrolidone (PVP) and poly(ethylene glycol) (PEG) with benign biocompatibility are commonly employed [34]. After proper chemical modification, these materials can be stimuli-responsive (pH, temperature, light and so on) and therefore endow MNAs with smart functions (e.g., spontaneously responding to blood glucose variation) [35, 36]. Compared to bulk MNAs, these MNAs present superior advantages of simple manufacture, low cost, and excellent biocompatibility, demonstrating the powerful capability of controllable drug delivery/release and stability/viability maintenance of living organisms.
In cases that living organisms need to retain inside MNAs to continuously secrete therapeutic agents and escape from the host immune response, insoluble MNAs encapsulating the creatures would be a preferred candidate owning to their biostability and porous structures. These MNAs are mainly made of insoluble hydrogels that can enclose therapeutic agents inside. Due to the porous and cage-like structure of the hydrogel, large payloads are retained inside the hydrogel while small molecules are continuously released outside, which can specifically regulate the secretion behavior of living species. For this purpose, the aforementioned biocompatible hydrogel is usually modified and crosslinked to be the insoluble form, providing long-term treatment. After penetrating target tissues, the MNAs spontaneously swell rather than dissolve, and thus maintain the organisms inside the MNAs while allow secretion to diffuse through the interspace of the hydrogel molecules.
MNAs integrated with living organisms
MNAs integrated with virus
Despite the tiny size (at the nanometer scale) and simple structures (only including nucleic acids and proteins), the viruses have been recognized as highly dangerous organisms given their high pathogenicity and infectivity [37, 38]. Numerous diseases relate to specific viruses, and some of them are still intractable, such as human immunodeficiency virus (HIV), Zika, coronavirus disease 2019 (COVID-19), and so on. Since Edward Jenner demonstrated the prevention of smallpox by prior infection with less dangerous cowpox virus in 1796 [39], the vaccine that utilizes exterior proteins/subunits of viruses to induce the virus recognition/clearance by the innate immune system, has been widely used to prevent virus-induced illness [40]. The conventional vaccine is mainly implemented via the hypodermic needle injection, which faces challenges including pain, cold-chain storage, hazardous sharps-waste, and the tremendous demand of trained medical personnel [41, 42]. MNAs, a promising alternative to needle injection, are painless, inexpensive and easy-for-use, which can act as an ideal tool for vaccine inoculation. Moreover, after adopting proper formulation, the virus vaccine loaded in MNAs can maintain long-term stability even in room temperature [43]. Besides vaccines, viruses have proven to work as vectors for gene delivery or direct tumor treatment [44-46]. After integration with MNA technology, the delivery of these kinds of viruses would be greatly improved, therefore facilitating gene therapies and tumor treatments. Applications using MNAs integrated with viruses are summarized in Table 1.
MNAs integrated with viruses
| Species | Microneedle arrays | Test subjects | Applications | References | ||
|---|---|---|---|---|---|---|
| Type (T)/Materials (M) | Height (H)/Diameter (D) | Array | ||||
| Recombinant MVA | T: Bulk M: Silicon | H: 100/125/200/300 μm D: - | 4 × 4 / 5 × 5 / 6 × 6 / 9 × 9 / 10 × 10 / 20 × 20 | Mice | Optimizing MNA design for vaccine delivery | [47] |
| Recombinant MVA/Recombinant AdHu5/Influenza X31 | T: Coated Core: Silicon Coating: Trehalose/maltodextrin/CMC/Tween 80 | H: 200/300 μm D: 100/150 μm | 4 × 4 / 6 × 6 | Mice | Developing spray-coating method for MNA-based vaccination | [48] |
| Recombinant AdHu5 | T: Dissolving M: Na-CMC/sucrose/lactose | H: 1500 μm D: 670 μm | 44 needles in 1 cm2 substrate | Mice | Preserving bioactivity of vaccines in MNAs and showing the immune response pathways | [49, 50] |
| Recombinant MVA/Recombinant ChAd63 | T: Coated Core: Silicon Coating: MC/PS20/trehalose/sucrose | H: 110 μm D: 22 μm | 58 × 58 | Mice | Evaluating long-term thermostability and immune response of dry-coated vaccine on MNAs | [51] |
| Recombinant MVA.ME-TRAP/Recombinant ChAd63.ME-TRAP | T: Bulk M: Silicon | H: 100/125/200/280/300 μm D: - | 4 × 4 / 6 × 6 / 9 × 9 / 10 × 10 / 20 × 20 | Mice | Malaria vaccine delivery by bulk MNAs | [52] |
| Recombinant AdHu5 | T: Dissolving M: Trehalose | H: 500 μm D: 300 μm | 5 × 5 | Mice | Malaria vaccine delivery by dissolving MNAs | [53] |
| Recombinant AdHu5 | T: Dissolving M: Na-CMC/sucrose/lactose | H: 1500 μm D: 670 μm | 44 needles in 1 cm2 substrate | Mice | Skin HIV vaccine delivery inducing mobilization of long lived, poly-functional CD8+ T cells | [54] |
| Adeno-associated-virus 9 | T: Insoluble M: PVA | H: 850 μm D: 334 μm | 44 needles in a substrate (Φ6 mm) | SD rat | Gene delivery for treating ischemic myocardial disease | [55] |
| Live-attenuated measles strain Edmonston-Zagreb | T: Coated Core: Stainless steel Coating: Trehalose/CMC/Lutrol F68 | H: 750 μm D: - | 5 needles in a row | Cotton rats | Measles vaccination through MNAs | [56] |
| Live-attenuated measles strain Edmonston-Zagreb | T: Dissolving M: Sucrose/threonine/CMC/PVA/PMMA | H: 600 μm D: 300 μm | 10 × 10 | Rhesus macaques | Measles vaccination through MNAs | [57] |
| Live-attenuated Edmonston-Zagreb measles strain and RA-27 rubella strain | T: Dissolving M: Sucrose/threonine/CMC/PVA | H: 700 μm D: - | 10 × 10 | Rhesus macaques | Delivering MR vaccine and accessing the immunogenicity | [58, 59] |
| Live-attenuated mumps virus/Live-attenuated varicella virus | T: Bulk M: Poly-glycolic acid | H: 700 μm D: 200 μm | 6 needles in a row | SD rat | Enhancing vaccine delivery and immune response | [60] |
| Live-attenuated dengue virus | T: Coated Core: Poly-L-lactide Coating: CMC/trehalose | H: 750 μm D: 250 μm | 77 needles (5 × 9 + 4 × 8) | Mice | Cold chain-independent dengue vaccine storage and delivery | [61] |
| Live vaccinia virus | T: Coated Core: PLA Coating: PVA/trehalose | H: 800 μm D: 370 μm | 97 needles in a substrate (Φ1 cm) | Mice | Evaluating the storage and inoculation of smallpox vaccine using MNAs | [62] |
| Cowpea mosaic virus | T: Dissolving M: PVP/Mg nanoparticles | H: 850 μm D: 400 μm | 15 × 15 | Mice | Melanoma treatment | [63] |
MVA: modified vaccinia virus Ankara; AdHu5: human adenovirus serotype 5; CMC: carboxymethyl cellulose; ChAd63: Simian adenovirus Chimpanzee serotype 63; MC: methyl cellulose; PS20: polysorbate 20; ME: Multiple epitope; TRAP: thrombospondin-related-adhesive-protein; SD rat: Sprague-Dawley rat; HIV: human immunodeficiency virus; MR: measles and rubella; PVP: polyvinyl pyrrolidone; PMMA: polymethyl methacrylate.
Recombinant viruses, which are alive but non-replicating, can be gene-edited by inserting exogenous genes that encode antigens of malaria, influenza, tuberculosis, HIV, and so on, serving as effective vaccines [64, 65]. For example, modified vaccinia virus Ankara (MVA) and replication-defective adenovirus (e.g., human adenovirus serotype 5 (AdHu5) and chimpanzee serotype 63 (ChAd63)) have been confirmed to be safe and immunogenic in human clinical trials [66, 67]. Vaccines from these living recombinant viral vectors have demonstrated great promise based on their capability to induce strong T-cell immunity [68, 69].
MNA technology has been widely applied for recombinant virus delivery to induce an intense immune response, and bulk MNAs are usually utilized given their excellent delivery efficiency. Moore et al. developed silicon MNAs with different dimension-related parameters, and compared their influence on the magnitude and memory of vaccine-induced CD8+ T cells [47]. Pearson et al. from the same research group also delivered an adenovirus-vectored malaria vaccine using the identical bulk MNAs, achieving corresponding results [52]. In the regime of bulk MNA delivery, vaccines were placed on the skin, followed by MNA treatment, which may lead to inconvenient operation and inaccurate dosage control. Therefore, coated MNAs became a more popular choice due to their low cost, one-step application and precise dose control. Intriguingly, Moore et al. investigated a spray-coating technique to load vaccines onto MNAs [48]. Different saccharides formulations were included to maintain the viral activity, acting as effective adjuvants. A similar investigation was implemented on MNA modified by dry-coating technology, and the data suggested the long-term thermostability of malaria vaccines loaded in MNAs over traditional ones [51]. Besides, dissolving MNAs were also employed to deliver recombinant viral vaccines due to their quick release and functional diversity. Klavinskis et al. adopted sodium carboxymethyl cellulose (Na-CMC) to fabricate a dissolving MNA containing AdHu5-vectored vaccine, which effectively exerted functions for at least one month. Their work also revealed the critical roles of different immune cells performed during the MNA vaccination (Figure 2A) [49]. A similar immune response was observed when applying dissolving MNAs to deliver vaccines against malaria and HIV [50, 53, 54].
Recombinant viruses integrated into MNAs. A (i) A dissolving MNA preserving the immunogenicity of dried AdHu5. (ii) Representative intravital confocal images of epidermis and dermis after MNA application, showing excellent MNA penetration into the skin with rapid dissolution. (iii) The MNA application-induced immunization response equipotent with conventional injected routes of vaccine delivery. Reproduced with permissions from National Academy of Society, USA 2013 [49]. B (i and ii) Ischemic hearts were treated by an MNA-encapsulating recombinant AAV9 which enabled gene transfection for enhancing VEGF expression, promoting functional angiogenesis and activating the Akt signaling pathway. (iii) MNAs delivered AAV-VEGF into the tissues of the infarction and enabled the local neovascularization. Reproduced with permissions from American Association for the Advancement of Science 2020 [55].
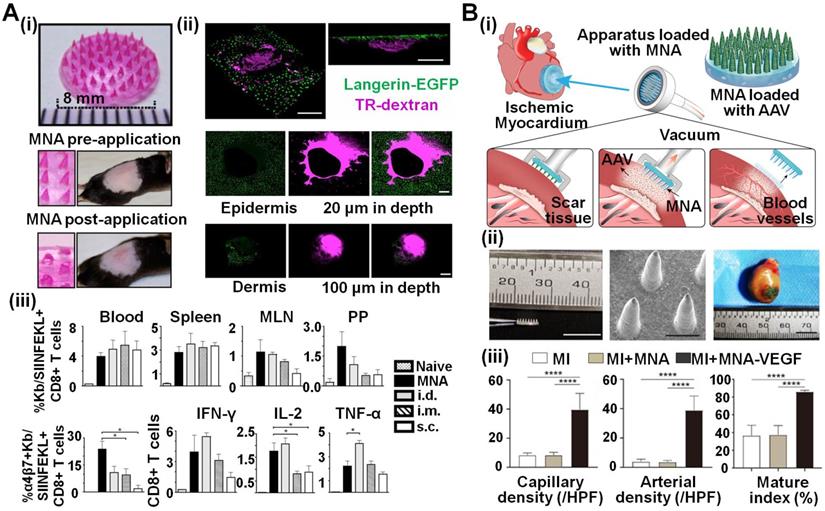
MNAs are also utilized to deliver recombinant viruses as gene carriers toward treating diseases based on gene therapy. Ye et al. engineered phase-transition MNAs loaded with adeno-associated virus (AAV) to deliver genes of vascular endothelial growth factor (VEGF) for cardiovascular disorder treatment (Figure 2B) [55]. The delivered AAV transfected cardiomyocytes in a homogeneous manner and was distributed evenly in the myocardiums. These MNAs significantly enhanced VEGF expression, promoted functional angiogenesis and thus improved heart functions in the ischemic area.
Besides recombinant viruses, natural viruses themselves have been broadly employed for infectious disease prevention and tumor treatment. Because replication competence and viral virulence do not frequently correlate with immunological robustness, live-attenuated viruses could also serve as potential vaccines. After attenuation, virus toxicity would decrease but their immunogenicity is reserved so that they can still trigger the immune response effectively [65]. Due to convenient operation and thermostability, attenuated virus-loaded MNAs remarkably improve vaccine storage and efficacy, especially in developing countries. Prausnitz et al. engineered MNAs to administer measles and rubella (MR) vaccine in rhesus macaques models (Figure 3A) [57-59]. With the help of sucrose-based MNAs, MR vaccines can be administered without well-trained personnel, resulting in fewer biohazardous sharp wastes and absent cold-chain storage. Similarly, various live-attenuated viruses including mumps, vaccinia and dengue have been successfully loaded in specific MNAs, and have proven to work as efficient vaccines [56, 60-62].
Live viruses integrated into MNAs used for vaccination or tumor treatment. A (i) Dissolving CMC MNAs containing live-attenuated Edmonston-Zagreb and RA-27 virus strains as the vaccine for measles and rubella. The MNAs made a minimal invasion on the skin (ii) while induced effective vaccination equipotent with subcutaneous injection and protected infant rhesus macaques from challenges with wild-type viruses (iii). Reproduced with permissions from Elsevier Limited 2020 [59]. B (i) In situ vaccination using an autonomous MNA for the treatment of B16F10 melanoma by releasing plant virus nanoparticles. (ii) The MNAs were fabricated using water-soluble polymer of PVP and contained Mg microparticles for active delivery of therapeutic CPMV nanoparticles. (iii) Tumor growth of melanoma on mice could be effectively suppressed, mainly by (iv) CPMV-induced in situ vaccination via enhancement of intratumor recruitment and activation of live CD45+ cells. Reproduced with permissions from American Chemical Society 2020 [63].
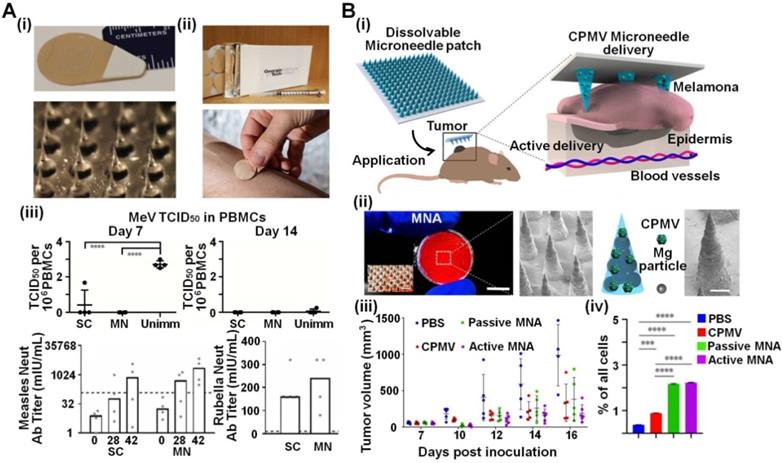
In addition to vaccines, viruses could also be applied to treat tumors (e.g., oncolytic viruses) [44]. Considering that MNAs can easily penetrate the skin, a combination of virus and MNAs to treat melanoma was implemented by Wang et al. (Figure 3B) [63]. They directly delivered cowpea mosaic virus (CPMV) intratumorally by MNA assisted by Mg nanoparticles, significantly suppressing canine melanoma in mice models. Notably, after delivery by dissolving MNAs, CPMV could intensively activate the innate immune system and recruit effecter T cells to suppress tumors. This work obviously confirmed the possibility of immune-mediated antitumor effects with the help of transdermal virus-integrated MNAs that can be easily implemented without professionals.
MNAs integrated with bacteria
It is well known that bacteria have shown a complicated relationship with human health for years [70]. Some so-called “probiotics” develop commensalism with human beings, and stay in organs such as the skin and gastrointestinal tract for a long time. Interestingly, they help human maintain homeostasis, digest food, provide unique metabolites and even benefit immunity. Meanwhile, there are still some bacteria causing various diseases especially when they are out of control [71-74]. However, those “harmful” bacteria can also be utilized to “train” our immune system to obtain specific immunity, suggesting potential infection prevention [75, 76]. Harnessing bacteria will undoubtedly benefit disease prevention and treatment with the help of artificial intervene. As the fast-developed approach for “smart” delivery of therapeutics, MNAs provide a facile and convenient tool to improve bacteria-based formulation in biomedical applications (Table 2).
MNAs integrated with living bacteria
| Species | Microneedle arrays | Test subjects | Applications | References | ||
|---|---|---|---|---|---|---|
| Type (T)/Materials (M) | Height (H)/Diameter (D) | Array | ||||
| C. albicans/P. aeruginosa/S. epidermidis | T: Bulk M: Silicon | H: 280 μm D: 250 μm | 6 × 7 | Excised porcine skin | Evaluating microbial penetration | [77] |
| E. coli DH5α | T: Bulk M: Metal | H: 200 / 500 / 1000 μm D: 80 μm | 7 needles per row (roller-like) | Hair-trimmed mouse skin | Evaluating potential risk of microbial infections | [78] |
| F. novicida | T: Bulk M: PLLA | H: 650 μm D: 250 μm | 7 × 11 | Mice | Inducing intradermal infections | [79] |
| Live-attenuated BCG bacillus | T: Dissolving M: HA | H: 200 μm D: 100 μm | 6 × 9 | Mice | Vaccine for tuberculosis | [80] |
| Lactobacillus | T: Dissolving M: SCMC | H: 600 μm D: 250 μm | 9 × 9 | Mice | Transdermal delivery of probiotics into local skin | [81] |
| B. subtilis | T: Insoluble M: PEGDA/PVA/HMPP | H: 500 μm D: 230 μm | 20 × 20 | Mice | Fungal infection treatment | [82] |
PLLA: Poly(L-lactide acid); BCG bacillus: Bacille Calmette-Guerin bacillus; HA: hyaluronate; SCMC: Sodium carboxymethyl cellulose; PEGDA: poly(ethylene glycol) diacrylate; PVA: polyvinyl alcohol; HMPP: 2-hydroxy-2-methylpropiophenone.
Living bacteria can be applied to evaluate the damage of the skin triggered by bulk MNAs. Donnelly et al. employed a silicon MNA on an in vitro model (excised porcine skin) to assess the infection potential of lesions compared with hypodermic needles [77]. They coated microbes (i.e., C. albicans, P. aeruginosa and S. epidermidis) on the surface of skin models and punctured the skin with hypodermic needles or MNAs. Subsequently, the number of bacteria in the skin was calculated to evaluate the possibility that organisms traversed the MNA-induced channels. Results obviously demonstrated that MNAs would not result in severe local or systemic infections, and thus validating the minimal invasion and safety of MNAs. Cui et al. obtained similar conclusions using a commercial MNA roller (Dermaroller®) made of metal (Figure 4A) [78]. In order to gain more information on how the delivered bacteria trigger the host response, Ernst et al. tested them in mice models (Figure 4B) [79]. F. novicida, a kind of bacteria that caused tularemia, was adhered onto a bulk MNA made of poly(L-lactide acid) (PLLA), and applied onto C57BL/6 mice. Successful bacteria deposition was observed, and survival rate and tissue response (in spleen, liver, lung and blood) such as T-cell depletion and inflammatory cytokine levels were monitored. Their results evidently showed that MNAs could effectively deliver bacteria into the skin to regulate immune responses in vivo.
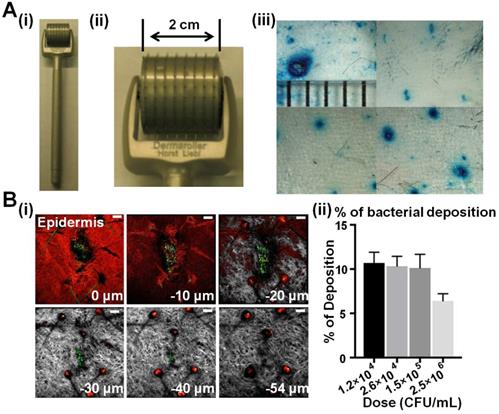
Bulk MNAs for intradermal bacteria permeation. A A commercial Dermaroller® MNA roller (i and ii) was used to evaluate E. coli DH5α penetration through MNA-treated mouse skin. (iii) Lesions made by a hypodermic needle and MNAs with needles of small (200 µm), medium (500 µm) and large (1000 µm) sizes were compared. Reproduced with permission from Dove Medical Press Limited 2011 [78]. B (i) Green fluorescent microspheres were employed to simulate F. novicida delivery to the ear skin of a DsRed-transgenic mouse using bulk PLLA MNAs, and (ii) the percentage of viable bacteria deposited from the MNA could be enumerated. Reproduced with permission from American Society for Microbiology 2018 [79].
With advances of biomaterials that could endow MNAs with smart functions like stimuli-responsiveness and sustained release, MNAs could be applied to significantly enhance bacteria-based therapies [29, 30]. For instance, aiming to popularize the inoculation of tuberculosis vaccine in areas with low economy and slow development, Wu et al. invented a dissolving MNA that contained caves near the bases of needles to store live-attenuated Bacille Calmette-Guerin (BCG) bacillus as a vaccine [80]. Tests showed that BCG bacillus could be stored for at least 90 days at room temperature, and was able to induce desirable immune protection, validated by intracellular cytokine productions and humoral responses in mice models. This MNA-based strategy exhibited similar inoculation efficiency compared to traditional intramuscular injection, while it did not require any medical professionals/equipment and cold-chain transportation, therefore facilitating popularization.
Other than being used as vaccines, bacteria, especially those probiotics, are also integrated into MNAs to treat skin diseases (e.g., fungal infection). Xie et al. encapsulated lactobacillus in the dissolvable sodium carboxymethyl cellulose and subsequently micromolded MNAs, followed by local delivery into the skin (Figure 5A). Results clearly showed that the probiotics inside the MNAs were kept alive at 4 ℃ for at least 21 days, and they could continuously produce lactic acid for 2 hours, and would not cause subcutaneous inflammation.
MNAs encapsulating therapeutic bacteria in a dissolving or hydrogel-forming manner. A (i) MNAs delivering bioactive functional probiotics into local skin to improve skin health and immunity. (ii) Lactobacillus as the model probiotic were encapsulated in the MNA tips. (iii) After insertion, the dissolved sodium carboxymethyl cellulose (SCMC, red fluorescence) and Lactobacillus (blue fluorescence) were deposited into the pig skin. Reproduced with permission from American Chemical Society 2018 [81]. B (i) A hydrogel-forming MNA encapsulating B. subtilis to release lipopeptides for treating fungal infection. (ii) The living bacteria stayed inside the MNAs without invasion and could be removed together with the patch. (iii) These MNAs showed effective capability when treating fungi-infected skin similar to ketoconazole. Reproduced with permission from American Association for the Advancement of Science 2020 [82].
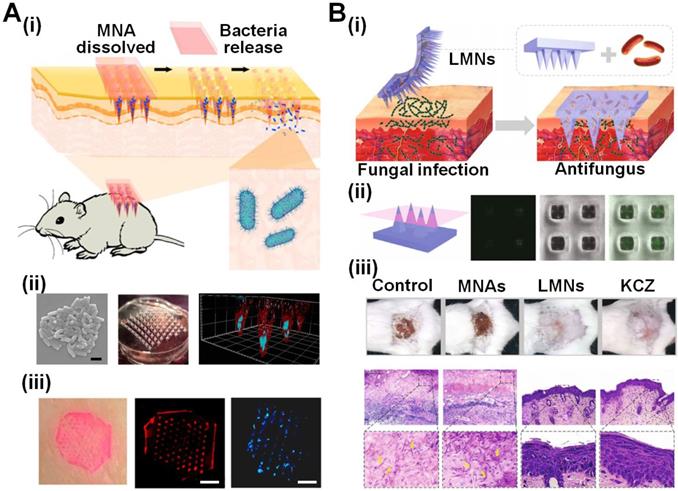
Given that some bacterial secretion may act as new agents to treat diseases [70, 71], bacteria are encapsulated in insoluble MNAs to continuously deliver bacterial secretion as therapeutic agents. These MNAs can trap the bacteria inside, and therefore avoid biosafety issues of uncontrolled bacterial proliferation when directly injecting bacteria into the human body. For example, considering the competition between beneficial bacteria and other microbes, Zhao et al. proposed a hydrogel-forming MNA that encapsulates living B. subtilis to secrete anti-fungal lipopeptides against C. albicans infection (Figure 5B) [82]. The beneficial bacteria were long-term maintained inside the MNAs and therefore would not cause an undesirable immune response, indicating a safe treatment. Importantly, this bacteria-MNA combinative strategy displayed similar antifungal effects compared to antibiotic ketoconazole, while showing no risk of drug resistance.
MNAs integrated with mammal cells
Recently, cell-based therapies emerge as a fast-growing field, and present great potential in tissue/organ repairing/regeneration and cancer treatment [14, 15]. However, traditional cell-based therapies are frequently compromised by low cell viability and immune rejection between hosts and the cells [83, 84]. How to achieve precise and controllable delivery of target cells in a convenient manner remains challenging.
Typical MNAs that could be employed for cell delivery are summarized in Table 3. Assisted by abundant functional materials, MNAs are able to encapsulate versatile cells and deliver them to various tissues, and therefore benefit the advance of point-of-care cell therapies. Based on the locations of the cells in the MNAs, these systems can be divided into cell-delivery MNAs and secretion-delivery MNAs.
MNAs integrated with living mammal cells
| Species | Microneedle arrays | Test subjects | Applications | References | ||
|---|---|---|---|---|---|---|
| Type (T)/Materials (M) | Height (H)/Diameter (D) | Array | ||||
| HaCaT Cells/Human follicle dermal papilla cells | T: Bulk M: PMMA | H: 1000 μm D: 200 μm | 6 × 6 | Collagen hydrogel | Cell delivery evaluation | [85] |
| Melanocyte/Keratinocyte/Epidermal cells | T: Bulk M: Silicon | H: 400/500/600/700 μm D: 200 μm | 5 × 5 | Excised human breast skin | Delivering functional cells for skin healing | [86] |
| Mardin-Darby canine kidney cells | T: Bulk M: SiO2/Si3N4 | H: 100/300/500 μm D: 30-50 μm | - | Rat liver tissue | Cell transplantation | [87] |
| B16-F10-murine-melanoma/HEK-293T cells | T:Dissolving M: HA/PVP/maltose | H: 650 μm D: 300 μm | 10 × 10 | Mice | In vivo tumor grafting | [88] |
| MSCs | T: Insoluble M: PLGA/GelMA | H: 700 μm H/D ratio = 1.5 | 8 × 8 | Mice | Wound repairing | [89] |
| RFP-HeLa/HaCaT/NDFs/MSCs/melanocytes/T cells/bone marrow-derived DCs/LPS-treated DCs | T: Dissolving M: PBS/DMSO/sucrose | H: 900 μm D: 350 μm | 10 × 10 | Mice | Transdermal delivery of therapeutic living cell | [90] |
| Pancreatic β-cells | T: Insoluble M: HA/alginate | H: 800 μm D: 400 μm | 20 × 20 | Mice | Type-1 diabetes treatment | [91] |
| CSCs | T: Insoluble M: PVA/fibrin gel | H: 600 μm D: 300 μm | 20 × 20 | Rat/Porcine | Heart regeneration after acute myocardial infarction | [92] |
| iPSC-derived cardiomyocytes | T: Insoluble M: GelMA/CNT | - | - | Mice | Treating acute myocardial infarction | [93] |
| CAR T cells | T: Solid M: PLGA | H: 1500 μm D: 250 μm | 15 × 15 | Mice | Seeding of CAR T cells for augmenting anticancer efficacy | [94] |
PMMA: polymethyl methacrylate; HA: hyaluronate; PVP: polyvinyl pyrrolidone; MSC: Mesenchymal stem cells; PLGA: poly(lactic-co-glycolic acid); GelMA: gelatin-methacryloyl; RFP: red fluorescent protein; NDF: Normal dermal fibroblast; DC: Dendritic cell; PBS: Phosphate buffer saline; DMSO: dimethylsulfoxide; CSC: cardiac stromal cell; PVA: polyvinyl alcohol; iPSC: induced pluripotent cell; CNT: carbon nanotube; CAR: chimeric antigen receptor.
Bulk MNAs have been attempted to deliver mammal cells by creating microchannels on the surfaces of target tissues. Huang et al. tried to deliver skin cells (keratinocytes HaCaT and human follicle dermal papilla cells) using bulk polymethyl methacrylate (PMMA) MNAs, which were successfully applied onto in vitro model (collagen hydrogel) [85]. Cells in suspension were laid and attached on the top of an MNA for 1-4 h and subsequently were transplanted to 2% collagen hydrogel by applying the MNA. The cell transplantation efficiency was around 80%, confirming the feasibility of cell delivery by bulk MNAs. And the cell viability could maintain at about 80% at Day 3 after delivery. Furthermore, cells could be delivered to the target through the channels inside the MNAs made of SiO2 or Si3N4 [86, 87]. Cellular viability and functions were evaluated to be similar to those injected by conventional hypodermic needles.
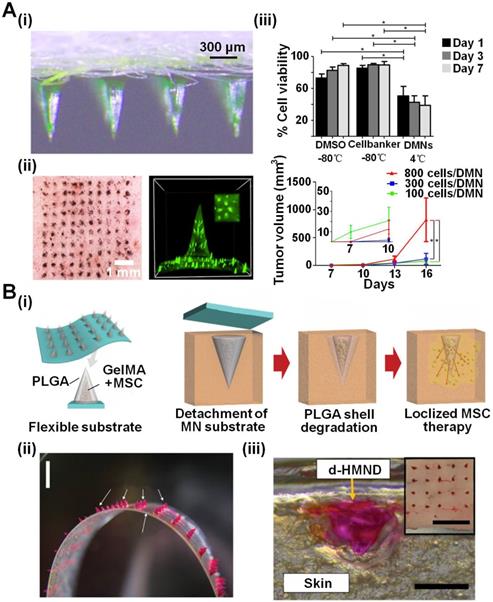
Compared to bulk MNAs, the utilization of biocompatible materials may provide high tunability to mediate cell behaviors. In these kinds of MNAs, cells were frequently encapsulated in needle tips and then were directly released in the tissues after penetration. For example, Wanichwecharungruang et al. utilized dissolving MNAs made of hyaluronate (HA)/polyvinyl pyrrolidone (PVP)/maltose to deliver cancer cells into mice models for tumor grafting (Figure 6A) [88]. After drying at 4 °C, the MNAs could maintain the viability of the encapsulated B16-F10-murine-melanoma at about 38.8% for 7 days. Cell transplantation using these B16-F10-cell-loaded MNAs displayed higher tumorigenesis efficiency and larger tumor graft compared to the hypodermic needle injection, possibly due to the temporary protection of HA/PVP/maltose on cells against host immune response. Khademhosseini et al. achieved localized MSC therapy using a similar cell-based dissolving MNA strategy (Figure 6B) [89]. Double-layered MNAs with needle tips that were comprised of a core made by gelatin-methacryloyl (GelMA) containing mesenchymal stem cells (MSCs) and poly(lactic-co-glycolic acid) (PLGA) shell, were employed to improve skin wound healing. After optimizing the fabrication process and constitutes, the MNAs presented superior mechanical property, and maintained the MSC viability over 90% for at least 24 h at 36.5 °C. Importantly, the encapsulated MSCs kept their stemness, and they could secrete vascular endothelial growth factor (VEGF) normally. When applied to the skin wounds, those MNAs showed enhanced healing ability with smaller wound areas, higher re-epithelialization, longer migrating epidermal tongue (MET), and greater CD31 intensity.
Transdermal delivery of living therapeutic cells using MNAs for cell-based therapies. A (i and ii) A dissolving MNA made of hyaluronate (HA)/polyvinyl pyrrolidone (PVP)/maltose delivering cancer cells into mice models for tumor grafting. (iii) The MNAs could maintain the viability of the encapsulated B16-F10-murine-melanoma at about 38.8% for 7 days. Cell transplantation using these B16-F10-cell-loaded MNAs displayed higher tumorigenesis efficiency and larger tumor formation using less cells compared to the hypodermic needle injection. Reproduced with permissions from American Chemical Society 2020 [88]. B (i) MSCs were delivered into localized skin by a core-shell MNA for would healing. (ii and iii) Cells were encapsulated in the GelMA hydrogel and coated by PLGA. When applied to mouse skin, PLGA dissolved and MSCs were left inside the target tissue. Cell viability could maintain 24 hours inside the MNA. Reproduced with permission from WILEY-VCH Verlag GmbH & Co. KgaA 2020 [89].
Another interesting transdermal cell delivery via MNAs was developed by Xu et al. using a cryogenic method [90]. The MNAs were fabricated by stepwise micromolding of cryogenic medium with pre-suspended cells, which could be readily inserted into porcine skin and dissolved after deployment of the cells. In vivo models validated that cells delivered by those cryomicroneedles remarkably retained their viability (ranging from 21.4% to 53.1%) and proliferative capability. In mice models with subcutaneous melanoma tumors, the delivery of ovalbumin-pulsed dendritic cells via the cryomicroneedles elicited higher antigen-specific immune responses and led to slower tumor growth compared to intravenous and subcutaneous injections of the cells. These biocompatible cryomicroneedles exhibited great potential to facilitate minimally invasive cell delivery and improve patients' compliance for a range of cell therapies (e.g., CAR T cell therapy [94]).
Other typical cell-based MNAs deliver not cells but their secretion (e.g., cytokines) into the pathological tissues to treat corresponding diseases. In those MNAs, functional cells are frequently encapsulated inside the base parts or on their surfaces, and thus are protected by cross-linked insoluble hydrogels against the host immune system. The needle tips of the MNAs create “microchannels” on the surfaces of target tissues and then the secreted therapeutic agents diffused through the microchannels to the pathological locations. Due to the continuously viability maintenance of the encapsulated cells, the cellular secretion persistently treats the lesions for a long time.
Considering the limitations of direct cell implantation for diabetes treatment such as host immunological rejection, Gu et al. encapsulated pancreatic β-cells in the MNA base made of HA/alginate hydrogel to achieve smart glucose response and insulin release, significantly improving Type-1 diabetes therapy (Figure 7A) [91]. They synthesized a kind of nanoparticles termed “glucose-signal amplifier” (GSA) which could sensitively respond to a hyperglycemic state and trigger the insulin secretion of pancreatic β-cells. This innovative GSA was featured with self-assembled polymeric nanosized vesicles entrapping three enzymes (glucose oxidase, α-amylase and glucoamylase), which overcome the limited glucose diffusion and finally amplified glucose signals, sensitizing pancreatic β-cell response. The recombination of cell therapy and smart-responsive materials helped those MNAs effectively regulate the blood glucose level in the streptozotocin (STZ)-induced type-1 mice.
MNAs encapsulating functional cells for releasing therapeutic agents to treat diseases. A (i) A Pancreatic β-cells integrated hydrogel-forming MNA to release insulin for treating diabetes in a smart responsive manner. Functional nanoparticles as glucose signal amplifiers sensed the blood glucose that diffused into the MNA and subsequently generated concentrated “amplified” glucose to trigger pancreatic β-cells for releasing insulin. (ii) The cell-based MNA penetration made less invasion in the skin while effectively regulate the blood glucose level in diabetes mouse models. Reproduced with permission from WILEY-VCH Verlag GmbH & Co. KgaA 2016 [91]. B (i and ii) A cardiac stromal cell integrated MNA treating myocardial infarction. (ii) Regenerative factors secreted by therapeutic CSCs seeded in the microneedle base could be transported to the injured myocardium through microneedle tips, enabling good cell retention and effective integration with host myocardium. Reproduced with permission from American Association for the Advancement of Science 2018 [92].
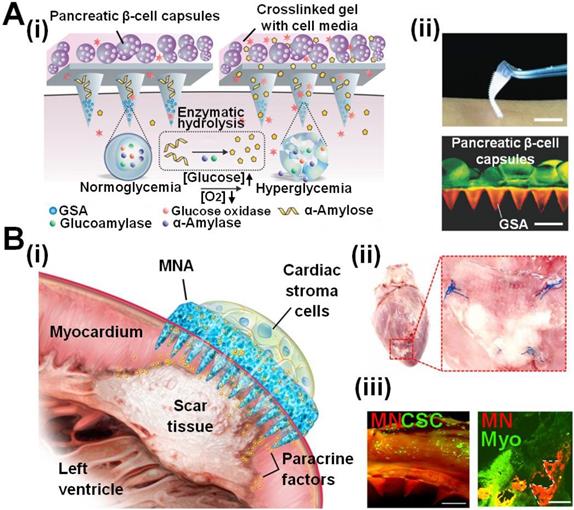
MNAs can provide ingenious strategies to improve cell-based therapies by preventing immune response and extending treatment periods, for example, in the field of curing heart diseases. Heart-derived cardiac stem/stromal cells can secrete regeneration factors to promote endogenous repair of the injured myocardium. However, the low cell viability by injection and the poor fusion with the host myocardium posed unique challenges for their applications. Cheng et al. developed polymeric MNAs integrated with cardiac stromal cells (CSCs) for therapeutic heart regeneration (Figure 7B) [92]. The MNAs provided multiple channels to allow communications between MNAs and the host myocardium. In this way, CSCs in the MNAs could obtain nutrients from the local environment while releasing paracrine factors to repair the heart. Those MNAs had proven to improve myocardial infarction (MI) treatment in experimental animals (rat and porcine), mainly by promoting angiomyogenesis, reducing scar size, and augmenting cardiac functions for 3 weeks. Other similar MNAs for MI treatment were developed by Zhao et al. which consisted of three layers: a drug-loaded MNA (bottom layer), parallel-aligned carbon nanotube (CNT) conductive (middle layer), and a methacrylated gelatin (GelMA) hydrogel scaffold (upper layer) [93]. iPSC-derived cardiomyocytes were laid and cultured on the surface of GelMA scaffolds, and could be kept viable and beating for at least 18 days. The secretion from integrated cells together with loaded cytokine drugs effectively promoted the regeneration and function recovery of MI hearts in mice.
Challenges and perspectives
Given the advantages of minimal invasion and easy operation, MNA technology has shown great potential in the fields of point-of-care drug administration, and convenient personalized diagnosis and therapies. Besides sampling biomarkers and delivering therapeutic agents, integrating with living organisms endows MNAs with versatile abilities from vaccination to cell-based therapies. Viruses, bacteria and mammal cells, whose size finely matches with micro-scaled MNAs, are ideal organisms employed in MNAs, showing high promise for either organism or secretion delivery. Those MNAs have been applied in various fields including but not limited to triggering adaptive immunity, treating infections or tumors, and repairing tissues, which provides convenient alternatives without professionals/equipment compared to traditional therapies based on drugs or surgeries.
Challenges
Although it has exhibited great potential, the integration of living organisms in MNAs still faces several challenges that limit their development:
(1) Maintaining bioactivity or viability of the integrated living organisms. Despite that various adjuvants (e.g., saccharides) have been adopted for long-term storage of virus-integrated MNAs, how to maintain the viability of more complicated organisms such as bacteria or cells in MNAs remains challenging. Recently, specific hydrogels or cryogenic reagents are under investigation, but they frequently require specific storage conditions of liquid nitrogen or humid incubators, which conflicts with the purposes of using MNAs as ordinary and convenient therapeutic tools in daily life.
(2) The biosafety of inducing living organisms into human beings. Since that MNAs either insert or directly implant into tissues, the contact between organisms and the human body lasts a period of time, either in a direct manner or separated by hydrogels. Therefore, the immunogenicity and the biosafety of those encapsulated organisms have to be considered. Certain organisms possess the ability of fast proliferation (e.g., the embedded bacteria or stem cells), and the infection or tumorigenesis will happen if their proliferation is out of control, posing risks to the host's health. Possible mutations of those evolving organisms during their fast growth, under a pathological environment or caused by implanted materials, might influence the organism's behaviors such as proliferation, differentiation, and so on [95, 96]. The behavior of originally encapsulated organisms is frequently under control, while the mutated organisms may proliferate immoderately (e.g., tumorigenesis due to gene mutation for cells). And the fast volume increase of these organisms as individual or group finally break the limitation of MNA structures, leading to their escape into the body and causing physical damages of the located tissues, excessive immune/inflammatory response or even death.
(3) Limited species of organisms and few locations for MNA application. Currently, only limited viruses, bacteria and cells are integrated with MNAs due to a lack of effective strategies and materials to hold organisms or regulate their behaviors. Moreover, current applications of MNAs are mainly restricted to the skin and heart tissues. Lack of feasible and practicable application or adhesion manners is the main reason that hinders the development of MNAs on other tissues.
Perspectives
In order to face the aforementioned challenges, attempts that devoted into following aspects are expected to further benefit human healthcare in a convenient, low-cost and point-of-care manner:
Integrating new species
Considering the versatile functions of extensive organisms and abundant biological tools developed to modify them, new species, besides the aforementioned viruses, bacteria and mammal cells, need to be tested in MNAs to seek novel strategies toward improving healthcare and treating diseases. For example, oxygen-producing algae can be utilized to remiss ischemic diseases that happened in the brain/heart [97] or to combat hypoxic tumors [98, 99]. In addition, phages that “eat” bacteria can help treat topical bacterial infections [100, 101]. Some other engineered bacteria can also be employed to treat tumors or gastrointestinal diseases [102-104]. Integrating MNAs with those organisms presents the potential for implementing fast and convenient organism-based therapies just at home and without the assistance of professionals.
Perspective of living organism-integrated MNAs. The MNAs could integrate new creature species, adopt new materials, expand applicable targets and combine new technologies to further benefit human healthcare in a convenient, low-cost and point-of-care manner.
Moreover, certain living creatures that possess immunogenicity could be applied to “train” the innate immune system to prevent various diseases. For instance, studies demonstrate that malaria infection can counteract tumor immunosuppressive microenvironment and inhibit the angiogenesis, growth and metastasis of tumors, which has been preliminarily validated by experiments on mice and human beings [105, 106]. It indicates the potential of delivering plasmodium by MNA as a non-invasive manner to combat certain cancers. Moreover, eggs of some parasites which are less virulent pathogenic are also able to trigger “vaccine-like” effects and reduce the risk of subsequent exposure to more pathogenic organisms [107, 108]. When being combined with delicate MNA strategies, the behavior and functions of those organisms can be well-regulated to facilitate medical applications.
In addition to the living species mentioned above, more organisms related to nutrition delivery and waste clearance could act as new candidates in MNA-biosystem combinations. For example, engineered bacteria/microalgae are expected to intake wastes such as CO2 or urea, and synthesize saccharides to supply nutrition to the target tissue. Furthermore, with the development of tissue engineering, many other human cells (e.g., kidney or liver cells) are anticipated to maintain viability inside MNAs, and then implanted to target tissues for metabolic waste clearance in a well regulatory profile.
Adopting new materials
Material science plays a significant role in MNA fabrication. Compared to traditional stiff materials with relatively sole functions (e.g., metal and silicon), abundant functional biomaterials, especially various natural or artificial polymers, have proven to significantly improve the performance of MNAs. Biocompatible materials have demonstrated the success of integrating living organisms with satisfactory viability inside MNAs by providing suitable microenvironments, for example, the adjuvant of saccharides is usually adopted to keep the virus stability when loading them into MNAs for vaccine inoculation. Biocompatible hydrogel (i.e., hyaluronate, polyvinyl alcohol) is mainly employed to encapsulate bacteria. During mammal cell encapsulation, the largest challenge is to maintain their viability in MNAs given the vulnerability of cells in vitro. One potential solution is to adopt special materials that are similar to the extracellular matrix for MNA fabrication, such as gelatin-methacryloyl (GelMA). Other methods focus on modifying reagents that are prepared for live cell storage at the low temperature, for example, the commonly-used cryogenic medium of dimethyl sulfoxide (DMSO) is incorporated with sucrose to balance between maintaining cell viability and realizing feasible MNA fabrication. What is more, new functionalized materials have drawn increasing attention in this field: (1) Besides biocompatibility, the newly-developed materials are expected to offer continuous nutrition supply, facilitating long-term creatures storage under room temperature or in a refrigerator. For example, extracts from silk (sericin and fibroin) are demonstrated to have a variety of biological activities for promoting cellular proliferation and inhibiting apoptosis, and thus benefit tissue regeneration [109-111]. Researchers have started to fabricate MNAs using this kind of material for wound recovery, drug delivery, vaccination and so on [112-114]. (2) The materials should not compromise the normal functions of the living organisms, given that the MNA matrix mainly serves as microenvironments for the encapsulated organisms. It is crucial to maintain the natural behaviors and metabolism of the organisms to avoid possible parasitosis or tumorigenesis. Furthermore, the new materials adopted are expected to be fine-tuned to actively program the behaviors of the integrated creatures, and therefore providing more flexible strategies. Considering biomolecules such as small peptides, glycans, and even proteins or polysaccharides, are able to provide signals that modulate cell adhesion, differentiation and development through interactions, they can be conjugated or modified on natural/artificial materials (e.g., gelatin, collagen, polyethylene glycol, poly(lactic acid) and so on) through covalent bonds and are able to direct cell behaviors [115, 116]. For example, PEG-based hydrogel with bone morphogenetic protein-2 (BMP-2) was employed as cell-ingrowth matrices for improving bone formation [117]. (3) In addition to the sufficient mechanical strength to insert target tissues, the long-term maintenance/adhesion of MNAs on the target surface is also required. Currently, when MNAs are needed to adhere to tissues for a long period of time, the suture is usually used, which may result in significant inconvenience and infections. Therefore, new materials with durable adhesion, will greatly improve the performance of MNAs [118, 119].
Expanding applicable targets
Since that MNA insertion requires extra pressure using applicators or thumb-pressing, current MNA-based systems are mainly limited to the skin and heart (during surgery). Therefore, developing new strategies based on MNA is urgently demanded. For instance, when being integrated with self-triggered spring [120] or magnetic guidance [121], MNAs can be delivered to the gastrointestinal (GI) tract, indicating an enteral delivery strategy. It is expected that after encapsulating proper bacteria, those MNAs can be used to regulate the intestinal microbes. Moreover, in combination with surgeries or interventional medicine, MNAs could be applied to more organs to treat diseases or maintain homeostasis after loading specific organisms [122]. For example, after being embedded with engineered liver cells, MNAs are able to attach to the liver during tumor excision surgeries, therefore helping to repair the organ or assist its functions (e.g., waste clearance). With the advances of interventional medicine techniques, specific catheters can go through natural lumens (e.g., arterial/venous vessels, gastrointestinal/biliary/urinary tract, etc.) and enable operations such as visualization, biopsy or minimally invasive surgery [123, 124]. After the proper design, MNAs are expected to be delivered to the heart, liver, kidney, stomach, intestine and so on by various catheters to realize potential minimally invasive organ treatment such as lesion repairing and tumor elimination.
Combining new technologies
With the development of biomedical technologies, MNA functionalization would be significantly enhanced to extend their applications. For instance, molecular imaging can be integrated with MNAs by encapsulating proper imaging agents (e.g., quantum dots and indocyanine green) inside MNAs, and thus facilitate visualization of pathological lesions as well as accurate medical recordkeeping [125, 126]. Loading other nanoparticles that have versatile functions such as responding to environment variation [127], carrying engineered biomolecules (e.g., DNA and RNA) [128, 129] and simulating cellular behaviors [130], can also enrich the functions of MNAs to improve their ability to regulate the integrated organisms.
Many emerging smart devices can be combined with MNAs as well. Microfluidics technology, acting as the newly emerging strategy to precisely control liquid motion in a small substrate [131, 132], can provide MNAs with fluid circulation capability, and therefore the MNAs are able to manipulate organism behavior by regulating the transport of nutrition and waste. Currently, several microfluidic systems combining with MNAs have been developed for various biomedical applications such as convenient and continuous injection and extraction [133], fluid management toward combinational therapy [134], and ISF collection facilitating biomarker analysis [135]. Moreover, the emerging “Organ on a chip” [136-138] and organoid technology [139, 140] enable simulation or even reconstruction of intact tissue/organ. When combining with MNA technology, the “Organ on a microneedle” may open a new window to improve organism-microneedle synergistic therapies.
Recently, the technology of wearable electronics has grown pretty fast and shown promising potential in monitoring the physical/physiological status of the human body [141-143]. The microscale and functional electronic devices can be implanted inside the bodies and communicate with daily-used smartphones [144, 145]. Various researches have demonstrated the integration of MNAs with those smart devices. And the applications mainly focus on the fields of real-time health monitoring and controllable transdermal drug delivery [146]. Similarly, MNAs would be functionalized to monitor the real-time performance of the encapsulated living organisms, ensuring the viability and status of the species. Furthermore, after assembly with microantennas to receive electric/photonic signals, and actuators (e.g., circuits or chemical reactors) to exert functions, the organism behaviors are expected to be finely tuned, indicating a highly regulatory fashion. When integrating with these techniques, the biggest advantage that MNAs can offer is the fast, convenient, and low-cost biomedical implementation without the assistance from professionals, which greatly benefits point-of-care diagnosis and therapies in a personal manner beyond hospitals.
Overall, microneedle arrays integrated with living organisms have exhibited great potential in the fields of point-of-care drug administration and personalized therapies in specific diseases. Those MNAs have proven to play a significant role in vaccination and cell therapy, especially for diseases related to immune disorders, infections, tumors, tissue damage, and so on, which are difficult to treat by traditional therapies (e.g., drugs or surgeries). With further development of biological, materials and engineering technologies, it is believed that the combination of living organisms with smart microneedle patches would hold great promise in the near future due to the advantages of both natural and artificial species.
Acknowledgements
The authors would like to acknowledge the support from the Fundamental Research Funds for the Central Universities (Grant No. 5003510106), and the National Natural Science Foundation of China (Grant No. 61904057, 82072167, 81873931, 81773104, 81974382).
Competing Interests
The authors have declared that no competing interest exists.
References
1. Clemente JC, Ursell LK, Parfrey LW, KR. The impact of the gut microbiota on human health: an integrative view. Cell. 2012;148:1258-70
2. Ding R-x, Goh W-R, Wu R-n, Yue X-q, Luo X, Khine WWT. et al. Revisit gut microbiota and its impact on human health and disease. J Food Drug Anal. 2019;27:623-31
3. Maizels RM, McSorley HJ. Regulation of the host immune system by helminth parasites. J Allergy Clin Immunol. 2016;138:666-75
4. Rauch S, Jasny E, Schmidt KE, Petsch B. New vaccine technologies to combat outbreak situations. Front Immunol. 2018;9:1963
5. Voigt EA, Kennedy RB, Poland GA. Defending against smallpox: a focus on vaccines. Expert Rev Vaccines. 2016;15:1197-211
6. Paul JP, Heather LD. History of vaccines and positioning of current trends. Curr Drug Targets Infect Disord. 2001;1:241-7
7. Imdad A, Nicholson MR, Tanner-Smith EE, Zackular JP, Gomez-Duarte OG, Beaulieu DB. et al. Fecal transplantation for treatment of inflammatory bowel disease. Cochrane Database Syst Rev. 2018;11:CD012774
8. D'Haens GR, Jobin C. Fecal Microbial transplantation for diseases beyond recurrent clostridium difficile infection. Gastroenterology. 2019;157:624-36
9. Lopetuso LR, Ianiro G, Allegretti JR, Bibbò S, Gasbarrini A, Scaldaferri F. et al. Fecal transplantation for ulcerative colitis: current evidence and future applications. Expert Opin Biol Ther. 2020;20:343-51
10. Squillaro T, Peluso G, Galderisi U. Clinical trials with mesenchymal stem cells: an update. Cell Transplant. 2016;25:829-48
11. Rowe RG, Daley GQ. Induced pluripotent stem cells in disease modelling and drug discovery. Nat Rev Genet. 2019;20:377-88
12. Wang Q, Cheng H, Peng H, Zhou H, Li PY, Langer R. Non-genetic engineering of cells for drug delivery and cell-based therapy. Adv Drug Deliv Rev. 2015;91:125-40
13. Sadelain M, Rivière I, Riddell S. Therapeutic T cell engineering. Nature. 2017;545:423-31
14. Guedan S, Ruella M, June CH. Emerging cellular therapies for cancer. Annu Rev Immunol. 2018;37:145-71
15. De Luca M, Aiuti A, Cossu G, Parmar M, Pellegrini G, Robey PG. Advances in stem cell research and therapeutic development. Nat Cell Biol. 2019;21:801-11
16. Bacakova L, Zarubova J, Travnickova M, Musilkova J, Pajorova J, Slepicka P. et al. Stem cells: their source, potency and use in regenerative therapies with focus on adipose-derived stem cells - a review. Biotechnol Adv. 2018;36:1111-26
17. Sarkar A, Saha S, Paul A, Maji A, Roy P, Maity TK. Understanding stem cells and its pivotal role in regenerative medicine. Life Sci. 2021;273:119270
18. Herberts CA, Kwa MSG, Hermsen HPH. Risk factors in the development of stem cell therapy. J Transl Med. 2011;9:29
19. Okano H, Nakamura M, Yoshida K, Okada Y, Tsuji O, Nori S. et al. Steps toward safe cell therapy using induced pluripotent stem cells. Circ Res. 2013;112:523-33
20. Zheng Z, Diaz-Arévalo D, Guan H, Zeng M. Noninvasive vaccination against infectious diseases. Hum Vaccin Immunother. 2018;14:1717-33
21. Feins S, Kong W, Williams EF, Milone MC, Fraietta JA. An introduction to chimeric antigen receptor (CAR) T-cell immunotherapy for human cancer. Am J Hematol. 2019;94:S3-S9
22. Mei X, Cheng K. Recent development in therapeutic cardiac patches. Front Cardiovasc Med. 2020;7:610364
23. Kwon H, Brown WE, Lee CA, Wang D, Paschos N, Hu JC. et al. Surgical and tissue engineering strategies for articular cartilage and meniscus repair. Nat Rev Rheumatol. 2019;15:550-70
24. Prausnitz MR. Engineering microneedle patches for vaccination and drug delivery to skin. Annu Rev Chem Biomol Eng. 2017;8:177-200
25. Moreira AF, Rodrigues CF, Jacinto TA, Miguel SP, Costa EC, Correia IJ. Microneedle-based delivery devices for cancer therapy: a review. Pharmacol Res. 2019;148:104438
26. Jamaledin R, Yiu CKY, Zare EN, Niu L-N, Vecchione R, Chen G. et al. Advances in antimicrobial microneedle patches for combating infections. Adv Mater. 2020;32:2002129
27. Amani H, Shahbazi M-A, D'Amico C, Fontana F, Abbaszadeh S, Santos HA. Microneedles for painless transdermal immunotherapeutic applications. J Control Release. 2021;330:185-217
28. Ma G, Wu C. Microneedle, bio-microneedle and bio-inspired microneedle: a review. J Control Release. 2017;251:11-23
29. Liu G-S, Kong Y, Wang Y, Luo Y, Fan X, Xie X. et al. Microneedles for transdermal diagnostics: recent advances and new horizons. Biomaterials. 2020;232:119740
30. Yang J, Liu X, Fu Y, Song Y. Recent advances of microneedles for biomedical applications: drug delivery and beyond. Acta Pharm Sin B. 2019;9:469-83
31. Dervisevic M, Alba M, Prieto-Simon B, Voelcker NH. Skin in the diagnostics game: wearable biosensor nano- and microsystems for medical diagnostics. Nano Today. 2020;30:100828
32. Lee KJ, Jeong SS, Roh DH, Kim DY, Choi H-K, Lee EH. A practical guide to the development of microneedle systems - in clinical trials or on the market. Int J Pharm. 2020;573:118778
33. Xie L, Zeng H, Sun J, Qian W. Engineering microneedles for therapy and diagnosis: a survey. Micromachines. 2020;11:271
34. Larrañeta E, Lutton REM, Woolfson AD, Donnelly RF. Microneedle arrays as transdermal and intradermal drug delivery systems: Materials science, manufacture and commercial development. Mater Sci Eng R Rep. 2016;104:1-32
35. Wei M, Gao Y, Li X, Serpe MJ. Stimuli-responsive polymers and their applications. Polym Chem. 2017;8:127-43
36. Shields Iv CW, Wang LL-W, Evans MA, Mitragotri S. Materials for Immunotherapy. Adv Mater. 2020;32:1901633
37. Sharp PM. Origins of human virus diversity. Cell. 2002;108:305-12
38. Rossmann MG. Structure of viruses: a short history. Q Rev Biophys. 2013;46:133-80
39. Hilleman MR. Six decades of vaccine development—a personal history. Nat Med. 1998;4:507-14
40. Akira S, Uematsu S, Takeuchi O. Pathogen recognition and innate immunity. Cell. 2006;124:783-801
41. Zipursky S, Djingarey MH, Lodjo J-C, Olodo L, Tiendrebeogo S, Ronveaux O. Benefits of using vaccines out of the cold chain: delivering meningitis a vaccine in a controlled temperature chain during the mass immunization campaign in Benin. Vaccine. 2014;32:1431-5
42. Simonsen L, Kane A, Lloyd J, Zaffran M, Kane M. Unsafe injections in the developing world and transmission of bloodborne pathogens: a review. Bull World Health Organ. 1999;77:789-800
43. Alcock R, Cottingham MG, Rollier CS, Furze J, De Costa SD, Hanlon M. et al. Long-term thermostabilization of live poxviral and adenoviral vaccine vectors at supraphysiological temperatures in carbohydrate glass. Sci Transl Med. 2010;2:19ra2-ra2
44. Lawler SE, Speranza M-C, Cho C-F, Chiocca EA. Oncolytic viruses in cancer treatment: a review. JAMA Oncol. 2017;3:841-9
45. Giacca M, Zacchigna S. Virus-mediated gene delivery for human gene therapy. J Control Release. 2012;161:377-88
46. Wang D, Tai PWL, Gao G. Adeno-associated virus vector as a platform for gene therapy delivery. Nat Rev Drug Discov. 2019;18:358-78
47. Carey JB, Pearson FE, Vrdoljak A, McGrath MG, Crean AM, Walsh PT. et al. Microneedle array design determines the induction of protective memory CD8+ T cell responses induced by a recombinant live malaria vaccine in mice. PLoS One. 2011;6:25
48. Vrdoljak A, McGrath MG, Carey JB, Draper SJ, Hill AVS, O'Mahony C. et al. Coated microneedle arrays for transcutaneous delivery of live virus vaccines. J Control Release. 2012;159:34-42
49. Bachy V, Hervouet C, Becker PD, Chorro L, Carlin LM, Herath S. et al. Langerin negative dendritic cells promote potent CD8+ T-cell priming by skin delivery of live adenovirus vaccine microneedle arrays. Proc Natl Acad Sci U S A. 2013;110:3041-6
50. Becker PD, Hervouet C, Mason GM, Kwon S-Y, Klavinskis LS. Skin vaccination with live virus vectored microneedle arrays induce long lived CD8+ T cell memory. Vaccine. 2015;33:4691-8
51. Pearson FE, McNeilly CL, Crichton ML, Primiero CA, Yukiko SR, Fernando GJP. et al. Dry-coated live viral vector vaccines delivered by nanopatch microprojections retain long-term thermostability and induce transgene-specific T cell responses in mice. PLoS One. 2013;8(7):e67888
52. Pearson FE, O'Mahony C, Moore AC, Hill AVS. Induction of CD8+ T cell responses and protective efficacy following microneedle-mediated delivery of a live adenovirus-vectored malaria vaccine. Vaccine. 2015;33:3248-55
53. Flynn O, Dillane K, Lanza JS, Marshall JM, Jin J, Silk SE. et al. Low adenovirus vaccine doses administered to skin using microneedle patches induce better functional antibody immunogenicity as compared to systemic injection. Vaccines. 2021;9:299
54. Zaric M, Becker PD, Hervouet C, Kalcheva P, Ibarzo Yus B, Cocita C. et al. Long-lived tissue resident HIV-1 specific memory CD8+ T cells are generated by skin immunization with live virus vectored microneedle arrays. J Control Release. 2017;268:166-75
55. Shi H, Xue T, Yang Y, Jiang C, Huang S, Yang Q. et al. Microneedle-mediated gene delivery for the treatment of ischemic myocardial disease. Sci Adv. 2020;6:eaaz3621
56. Edens C, Collins ML, Ayers J, Rota PA, Prausnitz MR. Measles vaccination using a microneedle patch. Vaccine. 2013;31:3403-9
57. Edens C, Collins ML, Goodson JL, Rota PA, Prausnitz MR. A microneedle patch containing measles vaccine is immunogenic in non-human primates. Vaccine. 2015;33:4712-8
58. Joyce JC, Carroll TD, Collins ML, Chen M-h, Fritts L, Dutra JC. et al. A microneedle patch for measles and rubella vaccination is immunogenic and protective in infant rhesus macaques. J Infect Dis. 2018;218:124-32
59. Prausnitz MR, Goodson JL, Rota PA, Orenstein WA. A microneedle patch for measles and rubella vaccination: a game changer for achieving elimination. Curr Opin Virol. 2020;41:68-76
60. Ogai N, Nonaka I, Toda Y, Ono T, Minegishi S, Inou A. et al. Enhanced immunity in intradermal vaccination by novel hollow microneedles. Skin Res Technol. 2018;24:630-5
61. Turvey ME, Uppu DSSM, Mohamed Sharif AR, Bidet K, Alonso S, Ooi EE. et al. Microneedle-based intradermal delivery of stabilized dengue virus. Bioeng Transl Med. 2019;4:e10127
62. Choi I-J, Cha H-R, Hwang SJ, Baek S-K, Lee JM, Choi S-O. Live vaccinia virus-coated microneedle array patches for smallpox vaccination and stockpiling. Pharmaceutics. 2021;13:209
63. Boone CE, Wang C, Lopez-Ramirez MA, Beiss V, Shukla S, Chariou PL. et al. Active microneedle administration of plant virus nanoparticles for cancer in situ vaccination improves immunotherapeutic efficacy. ACS Appl Nano Mater. 2020;3:8037-51
64. Hill AVS, Reyes-Sandoval A, O'Hara G, Ewer K, Lawrie A, Goodman A. et al. Prime-boost vectored malaria vaccines: progress and prospects. Hum Vaccines. 2010;6:78-83
65. Draper SJ, Heeney JL. Viruses as vaccine vectors for infectious diseases and cancer. Nat Rev Microbiol. 2010;8:62-73
66. Brookes RH, Hill PC, Owiafe PK, Ibanga HB, Jeffries DJ, Donkor SA. et al. Safety and immunogenicity of the candidate tuberculosis vaccine MVA85A in West Africa. PLoS One. 2008;3(8):e2921
67. Tatsis N, Ertl HCJ. Adenoviruses as vaccine vectors. Mol Ther. 2004;10:616-29
68. Barouch DH, Liu J, Li H, Maxfield LF, Abbink P, Lynch DM. et al. Vaccine protection against acquisition of neutralization-resistant SIV challenges in rhesus monkeys. Nature. 2012;482:89-93
69. Hansen SG, Ford JC, Lewis MS, Ventura AB, Hughes CM, Coyne-Johnson L. et al. Profound early control of highly pathogenic SIV by an effector memory T-cell vaccine. Nature. 2011;473:523-7
70. Cho I, Blaser MJ. The human microbiome: at the interface of health and disease. Nat Rev Genet. 2012;13:260-70
71. Lloyd-Price J, Abu-Ali G, Huttenhower C. The healthy human microbiome. Genome Med. 2016;8:51
72. Byrd AL, Belkaid Y, Segre JA. The human skin microbiome. Nat Rev Microbiol. 2018;16:143-55
73. Nicholson JK, Holmes E, Kinross J, Burcelin R, Gibson G, Jia W. et al. Host-gut microbiota metabolic interactions. Science. 2012;336:1262-7
74. Hooper LV, Littman DR, Macpherson AJ. Interactions between the microbiota and the immune system. Science. 2012;336:1268-73
75. Phadke VK, Bednarczyk RA, Salmon DA, Omer SB. Association between vaccine refusal and vaccine-preventable diseases in the United States: a review of measles and pertussis. JAMA. 2016;315:1149-58
76. Ottenhoff THM, Kaufmann SHE. Vaccines against tuberculosis: where are we and where do we need to go? PLoS Pathog. 2012;8(5):e1002607
77. Donnelly RF, Singh TRR, Tunney MM, Morrow DIJ, McCarron PA, O'Mahony C. et al. Microneedle arrays allow lower microbial penetration than hypodermic needles in vitro. Pharm Res. 2009;26:2513-22
78. Kumar A, Li XR, Sandoval MA, Rodriguez BL, Sloat BR, Cui ZR. Permeation of antigen protein-conjugated nanoparticles and live bacteria through microneedle-treated mouse skin. Int J Nanomed. 2011;6:2513-22
79. Chandler CE, Harberts EM, Laemmermann T, Zeng Q, Opene BN, Germain RN. et al. In vivo intradermal delivery of bacteria by using microneedle arrays. Infect Immun. 2018;86:e00406-18
80. Chen F, Yan Q, Yu Y, Wu MX. BCG vaccine powder-laden and dissolvable microneedle arrays for lesion-free vaccination. J Control Release. 2017;255:36-44
81. Chen H-J, Lin D-a, Liu F, Zhou L, Liu D, Lin Z. et al. Transdermal delivery of living and biofunctional probiotics through dissolvable microneedle patches. ACS Appl Bio Mater. 2018;1:374-81
82. Wang F, Zhang X, Chen G, Zhao Y. Living bacterial microneedles for fungal infection treatment. Research. 2020;2020:2760594
83. Ścieżyńska A, Soszyńska M, Szpak P, Krześniak N, Malejczyk J, Kalaszczyńska I. Influence of hypothermic storage fluids on mesenchymal stem cell stability: a comprehensive review and personal experience. Cells. 2021;10:1043
84. Liu X, Li W, Fu X, Xu Y. The immunogenicity and immune tolerance of pluripotent stem cell derivatives. Front Immunol. 2017;8:645
85. Chen Y-H, Lin D-C, Chern E, Huang Y-Y. The use of micro-needle arrays to deliver cells for cellular therapies. Biomed Microdevices. 2020;22:63
86. Gualeni B, Coulman SA, Shah D, Eng PF, Ashraf H, Vescovo P. et al. Minimally invasive and targeted therapeutic cell delivery to the skin using microneedle devices. Br J Dermatol. 2018;178:731-9
87. Iliescu FS, Teo JCM, Vrtacnik D, Taylor H, Iliescu C. Cell therapy using an array of ultrathin hollow microneedles. Microsyst Technol. 2018;24:2905-12
88. Pukfukdee P, Banlunara W, Rutwaree T, Limcharoen B, Sawutdeechaikul P, Pattarakankul T. et al. Solid composite material for delivering viable cells into skin tissues via detachable dissolvable microneedles. ACS Appl Bio Mater. 2020;3:4581-9
89. Lee K, Xue Y, Lee J, Kim H-J, Liu Y, Tebon P. et al. A patch of detachable hybrid microneedle depot for localized delivery of mesenchymal stem cells in regeneration therapy. Adv Funct Mater. 2020;30:2000086
90. Chang H, Chew SWT, Zheng M, Lio DCS, Wiraja C, Mei Y. et al. Cryomicroneedles for transdermal cell delivery. Nat Biomed Eng. 2021 DOI: 10.1038/s41551-021-00720-1
91. Ye Y, Yu J, Wang C, Nguyen N-Y, Walker GM, Buse JB. et al. Microneedles integrated with pancreatic cells and synthetic glucose-signal amplifiers for smart insulin delivery. Adv Mater. 2016;28:3115-21
92. Tang J, Wang J, Huang K, Ye Y, Su T, Qiao L. et al. Cardiac cell-integrated microneedle patch for treating myocardial infarction. Sci Adv. 2018;4:eaat9365
93. Sun L, Zhu X, Zhang X, Chen G, Bian F, Wang J. et al. Induced cardiomyocytes-integrated conductive microneedle patch for treating myocardial infarction. Chem Eng J. 2021;414:128723
94. Li H, Wang Z, Archibong E, Wu Q, Chen G, Hu Q. et al. Scattered seeding of CAR T cells in solid tumors augments anticancer efficacy. Natl Sci Rev. 2021 DOI: 10.1093/nsr/nwab172
95. Doss MX, Sachinidis A. Current challenges of iPSC-based disease modeling and therapeutic implications. Cells. 2019;8:403
96. Musiał-Wysocka A, Kot M, Majka M. The pros and cons of mesenchymal stem cell-based therapies. Cell Transplant. 2019;28:801-12
97. Wang J, Su Q, Lv Q, Cai B, Xiaohalati X, Wang G. et al. Oxygen-generating cyanobacteria powered by upconversion-nanoparticles-converted near-infrared light for ischemic stroke treatment. Nano Lett. 2021;21:4654-65
98. Zhong D, Zhang D, Xie T, Zhou M. Biodegradable microalgae-based carriers for targeted delivery and imaging-guided therapy toward lung metastasis of breast cancer. Small. 2020;16:2000819
99. Zhong D, Li W, Hua S, Qi Y, Xie T, Qiao Y. et al. Calcium phosphate engineered photosynthetic microalgae to combat hypoxic-tumor by in-situ modulating hypoxia and cascade radio-phototherapy. Theranostics. 2021;11:3580-94
100. Fathima B, Archer AC. Bacteriophage therapy: recent developments and applications of a renaissant weapon. Res Microbiol. 2021: 103863.
101. Wu N, Zhu T. Potential of therapeutic bacteriophages in nosocomial infection management. Front Microbiol. 2021 12
102. Cao Z, Cheng S, Wang X, Pang Y, Liu J. Camouflaging bacteria by wrapping with cell membranes. Nat Commun. 2019;10:3452
103. Wang X, Cao Z, Zhang M, Meng L, Ming Z, Liu J. Bioinspired oral delivery of gut microbiota by self-coating with biofilms. Sci Adv. 2020;6:eabb1952
104. Li Z, Wang Y, Liu J, Rawding P, Bu J, Hong S. et al. Chemically and biologically engineered bacteria-based delivery systems for emerging diagnosis and advanced therapy. Adv Mater. 2021;33:2102580
105. Greentree LB. Malariotherapy and cancer. Med Hypotheses. 1981;7:43-9
106. Chen X, Qin L, Hu W, Adah D. The mechanisms of action of Plasmodium infection against cancer. Cell Commun Signal. 2021;19:74
107. Pearce EJ. Priming of the immune response by schistosome eggs. Parasite Immunol. 2005;27:265-70
108. Carson JP, Gobert GN. Modulation of the host immune response by schistosome egg-secreted proteins is a critical avenue of host-parasite communication. Pathogens. 2021;10:863
109. Song Y, Wang H, Yue F, Lv Q, Cai B, Dong N. et al. Silk-basedbiomaterials for cardiac tissue engineering. Adv Healthc Mater. 2020;9:2000735
110. Wang Z, Wang J, Jin Y, Luo Z, Yang W, Xie H. et al. A neuroprotective sericin hydrogel as an effective neuronal cell carrier for the repair of ischemic stroke. ACS Appl Mater Interfaces. 2015;7:24629-40
111. Wang J, Li X, Song Y, Su Q, Xiaohalati X, Yang W. et al. Injectable silk sericin scaffolds with programmable shape-memory property and neuro-differentiation-promoting activity for individualized brain repair of severe ischemic stroke. Bioact Mater. 2021;6:1988-99
112. Stinson JA, Boopathy AV, Cieslewicz BM, Zhang Y, Hartman NW, Miller DP. et al. Enhancing influenza vaccine immunogenicity and efficacy through infection mimicry using silk microneedles. Vaccine. 2021;39:5410-21
113. Yavuz B, Chambre L, Harrington K, Kluge J, Valenti L, Kaplan DL. Silk fibroin microneedle patches for the sustained release of levonorgestrel. ACS Appl Bio Mater. 2020;3:5375-82
114. Gao B, Guo M, Lyu K, Chu T, He B. Intelligent silk fibroin based microneedle dressing (i-SMD). Adv Funct Mater. 2021;31:2006839
115. Murphy WL, McDevitt TC, Engler AJ. Materials as stem cell regulators. Nat Mater. 2014;13:547-57
116. Nicolas J, Magli S, Rabbachin L, Sampaolesi S, Nicotra F, Russo L. 3D extracellular matrix mimics: fundamental concepts and role of materials chemistry to influence stem cell fate. Biomacromolecules. 2020;21:1968-94
117. Lutolf MP, Weber FE, Schmoekel HG, Schense JC, Kohler T, Müller R. et al. Repair of bone defects using synthetic mimetics of collagenous extracellular matrices. Nat Biotechnol. 2003;21:513-8
118. Yuk H, Varela CE, Nabzdyk CS, Mao X, Padera RF, Roche ET. et al. Dry double-sided tape for adhesion of wet tissues and devices. Nature. 2019;575:169-74
119. Inoue A, Yuk H, Lu B, Zhao X. Strong adhesion of wet conducting polymers on diverse substrates. Sci Adv. 2020;6:eaay5394
120. Abramson A, Caffarel-Salvador E, Khang M, Dellal D, Silverstein D, Gao Y. et al. An ingestible self-orienting system for oral delivery of macromolecules. Science. 2019;363:611-5
121. Zhang X, Chen G, Fu X, Wang Y, Zhao Y. Magneto-responsive microneedle robots for intestinal macromolecule delivery. Adv Mater. 2021 2104932
122. Lee K, Goudie MJ, Tebon P, Sun W, Luo Z, Lee J. et al. Non-transdermal microneedles for advanced drug delivery. Adv Drug Deliv Rev. 2020;165-166:41-59
123. Schoenberg SO, Attenberger UI, Solomon SB, Weissleder R. Developing a roadmap for interventional oncology. Oncologist. 2018;23:1162-70
124. Shafiq M, Lee H, Yarmus L, Feller-Kopman D. Recent advances in interventional pulmonology. Ann Am Thorac Soc. 2019;16:786-96
125. McHugh Kevin J, Jing L, Severt Sean Y, Cruz M, Sarmadi M, Jayawardena Hapuarachchige Surangi N. et al. Biocompatible near-infrared quantum dots delivered to the skin by microneedle patches record vaccination. Sci Transl Med. 2019;11:eaay7162
126. Kwon S, Velasquez FC, Rasmussen JC, Greives MR, Turner KD, Morrow JR. et al. Nanotopography-based lymphatic delivery for improved anti-tumor responses to checkpoint blockade immunotherapy. Theranostics. 2019;9:8332-43
127. Qin W, Quan G, Sun Y, Chen M, Yang P, Feng D. et al. Dissolving Microneedles with Spatiotemporally controlled pulsatile release Nanosystem for Synergistic Chemo-photothermal Therapy of Melanoma. Theranostics. 2020;10:8179-96
128. Huang D, Zhao D, Wang X, Li C, Yang T, Du L. et al. Efficient delivery of nucleic acid molecules into skin by combined use of microneedle roller and flexible interdigitated electroporation array. Theranostics. 2018;8:2361-76
129. Liao J-F, Lee J-C, Lin C-K, Wei K-C, Chen P-Y, Yang H-W. Self-Assembly DNA Polyplex Vaccine inside Dissolving Microneedles for High-Potency Intradermal Vaccination. Theranostics. 2017;7:2593-605
130. Zeng Y, Zhou H, Ding J, Zhou W. Cell membrane inspired nano-shell enabling long-acting Glucose Oxidase for Melanoma starvation therapy via microneedles-based percutaneous delivery. Theranostics. 2021;11:8270-82
131. Sackmann EK, Fulton AL, Beebe DJ. The present and future role of microfluidics in biomedical research. Nature. 2014;507:181-9
132. Zhong Q, Ding H, Gao B, He Z, Gu Z. Advances of Microfluidics in Biomedical Engineering. Adv Mater Technol. 2019;4:1800663
133. Trautmann A, Roth G-L, Nujiqi B, Walther T, Hellmann R. Towards a versatile point-of-care system combining femtosecond laser generated microfluidic channels and direct laser written microneedle arrays. Microsyst Nanoeng. 2019;5:6
134. Yeung C, Chen S, King B, Lin H, King K, Akhtar F. et al. A 3D-printed microfluidic-enabled hollow microneedle architecture for transdermal drug delivery. Biomicrofluidics. 2019;13:064125
135. Takeuchi K, Takama N, Kim B, Sharma K, Paul O, Ruther P. Microfluidic chip to interface porous microneedles for ISF collection. Biomed Microdevices. 2019;21:28
136. Low LA, Mummery C, Berridge BR, Austin CP, Tagle DA. Organs-on-chips: into the next decade. Nat Rev Drug Discov. 2021;20:345-61
137. Jalili-Firoozinezhad S, Miranda CC, Cabral JMS. Modeling the human body on microfluidic chips. Trend Biotechnol. 2021;39:838-52
138. Zhang P, Shao N, Qin L. Recent Advances in microfluidic platforms for programming cell-based living materials. Adv Mater. 2021: 2005944.
139. Schutgens F, Clevers H. Human organoids: tools for understanding biology and treating diseases. Annu Rev Pathol Mech Dis. 2020;15:211-34
140. Li M, Izpisua Belmonte JC. Organoids — preclinical models of human disease. N Engl J Med. 2019;380:569-79
141. Shrivastava S, Trung TQ, Lee N-E. Recent progress, challenges, and prospects of fully integrated mobile and wearable point-of-care testing systems for self-testing. Chem Soc Rev. 2020;49:1812-66
142. Ma Y, Zhang Y, Cai S, Han Z, Liu X, Wang F. et al. Flexible hybrid electronics for digital healthcare. Adv Mater. 2020;32:1902062
143. Shi Q, Dong B, He T, Sun Z, Zhu J, Zhang Z. et al. Progress in wearable electronics/photonics—moving toward the era of artificial intelligence and internet of things. InfoMat. 2020;2:1131-62
144. Lou Z, Wang L, Jiang K, Wei Z, Shen G. Reviews of wearable healthcare systems: Materials, devices and system integration. Mater Sci Eng R Rep. 2020;140:100523
145. Shih B, Shah D, Li J, Thuruthel TG, Park Y-L, Iida F. et al. Electronic skins and machine learning for intelligent soft robots. Sci Robot. 2020;5:eaaz9239
146. Teymourian H, Tehrani F, Mahato K, Wang J. Lab under the skin: microneedle based wearable devices. Adv Healthc Mater. 2021;10:2002255
Author contact
![]() Corresponding authors: Zheng Wang (E-mail: zhengwangedu.cn); Lin Wang (E-mail: lin_wangedu.cn); Wei Chen (E-mail: weichen86edu.cn).
Corresponding authors: Zheng Wang (E-mail: zhengwangedu.cn); Lin Wang (E-mail: lin_wangedu.cn); Wei Chen (E-mail: weichen86edu.cn).